Authors: Jay T. Sutliffe, Julia C. Gardner, Jenny M. Gormley, Mary Jo. Carnot, and Alison Adams
Corresponding Author:
Jay Sutliffe, PhD, RD
PO Box 15095
Flagstaff AZ, 86011
Jay.sutliffe@nau.edu
928-523-7596
Jay T. Sutliffe is Associate Professor of Nutrition and Foods and the Director of the PRANDIAL Lab at Northern Arizona University in Flagstaff, AZ; Julia C. Gardner is a research coordinator with the PRANDIAL Lab at Northern Arizona University; Mary Jo Carnot is professor of Counseling, Psychological Sciences, and Social Work at Chadron State College in Chadron, NE.; Jenny M. Gormley is a research assistant and student at Northern Arizona University; Alison Adams, is Professor of Biology at Northern Arizona University.
Assessing the Dietary Quality and Health Status Among Division 1 College Athletes at Moderate Altitude
ABSTRACT
Student-athletes’ dietary habits are ingrained in a complex interaction as they seek to maintain the balance between student and athlete. Assessing the dietary habits and lifestyle factors associated with this highly demanding population is the focus of this study. Eighty-nine Division I Collegiate Athletes was assessed (age 19.84 ± 1.15 yr). Measurements included diet quality, body composition, blood lipid profiling, and wellness factors. Significant deficiencies in Vitamin D (football 6.68 ± 5.84; basketball 4.33 ± 3.17; swim/dive 4 ± 2.97; volleyball 4.07 ± 2.97) and Omega 3-EPA & DHA (football 125.84 ± 301.03; basketball 53.92 ± 48.05; swim/dive 29.45 ± 35.83; volleyball 42.79 ± 30.77), Calcium (swim/dive 1083.55 ± 437.88), and Potassium (swim/dive 1083.55 ± 437.88) were reported. All teams exhibited an energy deficit, however, the highest energy deficit was for football (-843.57 calories). All teams had higher than recommended levels of perceived stress, averaging 20.63, and swim/dive had higher levels of depressive symptoms (6.17 ± 3.30). All teams reported poor sleep quality, averaging 7.20. This assessment indicates variability in dietary quality and wellness factors among individuals and teams. Individualized guidelines should be recommended for those experiencing food intake challenges such as the unique needs of moderate altitude athletes.
Keywords: micronutrients, nutrition intervention, athlete, body-composition, altitude
INTRODUCTION
Student-athlete diets are often lacking in variety, micronutrients, and are typically high in processed foods, refined fatty foods, and simple carbohydrates (3, 10, 17). Additionally, student-athlete energy intake is often inadequate to support strenuous training regimens due to consumption of insufficient calories to fuel energy expenditure, potentially leading to low energy availability. Prolonged low energy availability may subsequently result in inadequate micronutrient consumption. Regular and ongoing suboptimal intakes of vitamins and minerals may result in a reduction in work performance and endurance, delayed recovery, impaired muscle function, increased ventilation and heart rate, increased risk of disease, and limited work capacity (25, 26). Micronutrients are key components of all human metabolic processes including immunity, inflammation, and recovery and the recommended intake significantly increases with athletic training and competition.
At moderate altitude, there may be specific altitude-related effects for student-athletes in relation to energy needs and expenditure, hydration status, dietary carbohydrate intake, antioxidant needs, iron storage, vitamin D, the B vitamins, and other non-nutritional wellness aspects (28). Additionally, the demands of altitude may lead to hypoxia and appetite suppression while corresponding basal metabolic rates may increase, resulting in the gradual reduction in body weight and muscle mass (11).
In the current study, dietary quality, serum lipid profiles, body composition and related anthropometric measures, hydration status, blood pressure, and well-being measures such as sleep, perceived stress, and depressive symptoms were assessed in Division 1 collegiate student-athletes at moderate altitude (5,000-8,000 feet above sea level) (12).
Materials and Methods
Participants
Volunteers were recruited from the student-athlete population at a National Collegiate Athletic Association (NCAA) Division I program situated at approximately 7,000 feet above sea level. All participants were involved in 1-3 hours/day of moderate to high-intensity exercise most days. Of eighty-nine participants enrolled, 74.16 % were male and 25.84 % female. Participants represented the following sport teams: men’s football (61.80 %), men’s basketball (12.36 %), women’s volleyball (10.11 %) and women’s swim/dive (15.73 %) with a mean age 19.84 ± 1.15 years. Several ethnicities were represented: 56.1% Caucasian, 28.09% African American, 6.74% South American, and 1.12% Southeast Asian. Overall, the sample represents 25.4% of the total student-athlete population for 2017 (29). No exclusionary health criteria were developed for this study, as all NCAA student-athletes are required to complete yearly athletic physicals to screen for possible health risks. The study was approved by the Institutional Review Board (IRB ID 982568) and all participants provided informed consent.
Study Design
The purpose of this study was to determine dietary quality, food frequency, body composition, anthropometric, blood-lipid, and well-being status of NCAA Division 1 American student-athletes living, training, and competing at moderate altitude.
Diet Quality and Assessment
Using the direct interview method at the Laboratory for Exercise and Nutrition (LEAN Lab), trained interviewers collected 24-Hour Dietary Recall (24HR) and one-week Food Frequency Questionnaire (FFQ) from each participant (1). The 24HR is a nutrition assessment method recalling foods and beverages consumed in the twenty-four hours prior to the interview. The 24HR is a commonly used method for dietary assessment and has been validated for use with athletes (2). Since the 24HR is unable to account for day-to-day variation, the FFQ was also used. The FFQ is a dietary survey method that places minimal burden on participants and documents general food consumption patterns over the past week or month. The FFQ has been shown to have validity among young athletes (36).
For both the 24HR and FFQ, to increase accurate and specific recall, Nasco food models/replicas were utilized to confirm specific portions of the food and beverages consumed; Nasco, Fort Atkinson, Wisconsin, USA. The data from these interviews were then entered into the online United States Department of Agriculture (USDA) SuperTracker tool by a member of the research team.
The USDA SuperTracker is an online food tracking tool designed to provide an accurate assessment of dietary intake and quality (Supertracker.usda.gov). This software provides a comparison between the participants’ actual dietary consumption and the Dietary Guidelines for Americans based on activity level. The comparison is provided in a nutrient intake report, providing information for calories, macronutrients, and micronutrients. NOTE: The SuperTracker tool was discontinued June 30, 2018.
Blood-Lipid Analysis
A blood-lipid profile, performed by trained technicians, was conducted after participants fasted for a minimum of 8-hours, and performed at 6:30 – 9:30 A.M. The technician’s utilized 35-ml capillary whole blood specimens obtained by finger stick applied to the Clinical Laboratory Improvement Amendments (CLIA) waived Alere Cholestech LDX System Analyzer; Alere, Abbott Rapid Diagnostics, Illinois, USA.
Anthropometric and Body-Composition Measurements
Evaluation of body composition was conducted using tetrapolar bioelectrical impedance analysis (BIA); BIA; Seca® mBCA 515, HANS E. RÜTH S.A., Hamburg, Germany. BIA is an efficient and non-invasive technique that enables determination of body composition based on the measurement of electrical characteristics of the human body by body region. Regions included left and right arms and legs, and the torso. These data can be used to assess metabolic activity, energy consumption, energy reserves, fluid status, and abdominal fat (Visceral Adipose Tissue, VAT). Phase angle (phA) in BIA is a validated measurement that correlates with percentage body fat (%BF), body mass index (BMI), fat mass (FM), and total body water (TBW) (22). A low phase angle by BIA is associated with increased morbidity and nutritional risk (23,32). However, anthropometric measurements also need to be considered, since phA is affected by body geometry as well. Individuals with hydration outliers i.e., unstable extracellular water (ECW) and intracellular water (ICW) ratios can obtain a phase angle measurement when using bioelectrical impedance vector analysis (BIVA), which uses the plot resistance and reactance normalized per height (21,33).
Well-being Measures
Well-being data were collected and managed using the Research Electronic Data Capture (REDCap) electronic data tool (14). REDCap is a secure web application for building and managing online surveys and databases. It is designed to support online or offline data capture for any type of data including 21 CFR Part 11 and Health Insurance Portability and Accountability Act (HIPAA) compliant environments.
The following self-reported well-being measures were collected electronically: Patient Health Questionnaire (PHQ-9) (20) for depressive symptoms, the Pittsburgh Sleep Quality Index (PSQI) (8), Perceived Stress Scale (PSS) (9), and the Gastroesophageal Reflux Disease (GERD) Questionnaire (GerdQ) (16).
Statistical Analysis
Descriptive statistics were used to describe the basic characteristics of the data using Software for Statistics and Data Science (STATA) software version 15.1; StataCorp LLC, College Station, Texas, USA. SYSTAT version 13 was used for other analyses; Systat Software Inc., San Jose, California, USA. For most variables, descriptive data only are of interest in establishing measures of diet and nutrition for student-athletes. Comparisons to RDI were completed using single sample t tests, with an alpha level of .01.
RESULTS
Table 1 describes the various components related to energy balance by sport. The results reveal that none of the sports teams consumed adequate energy to cover the energy requirements represented by their estimated total energy expenditure. Of the teams represented, football showed the largest deficit of energy of 843.57 calories per day.
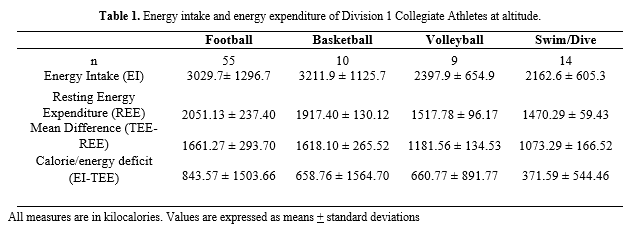
Table 2 indicates average macronutrient and related consumption by sport. On average, all teams consumed adequate amounts of protein. For football, carbohydrate and fiber consumption was low, and total fats, saturated fats were higher than recommended for male athletes. Cholesterol intake was higher than recommended for three of the four teams with football consuming nearly double the recommended amount. Omega-3 fatty acid consumption was very low for all teams.
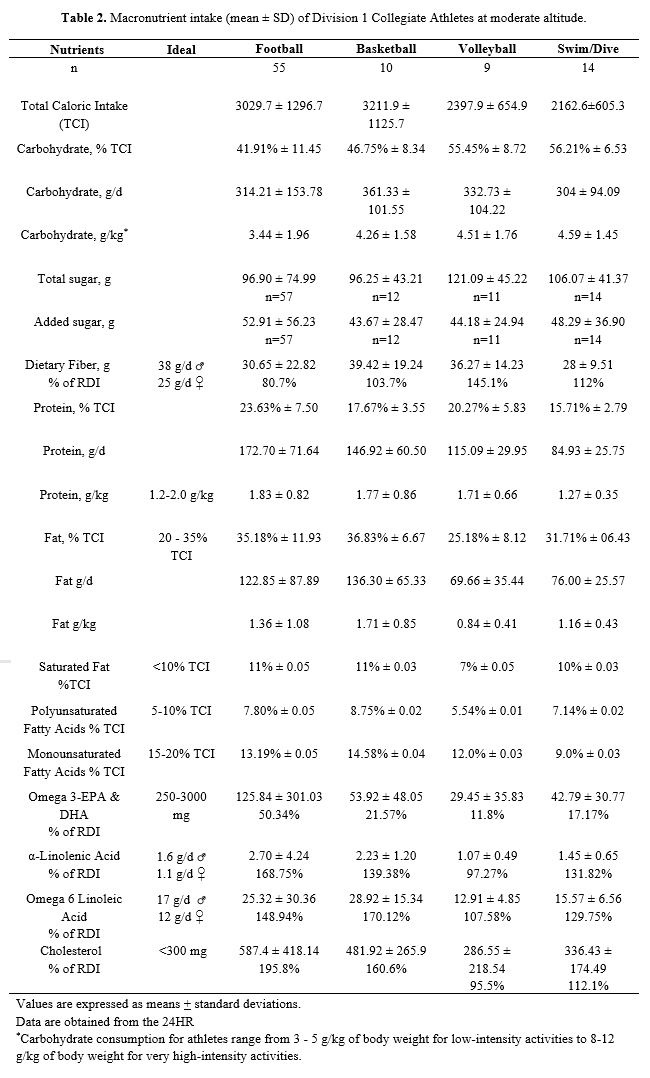
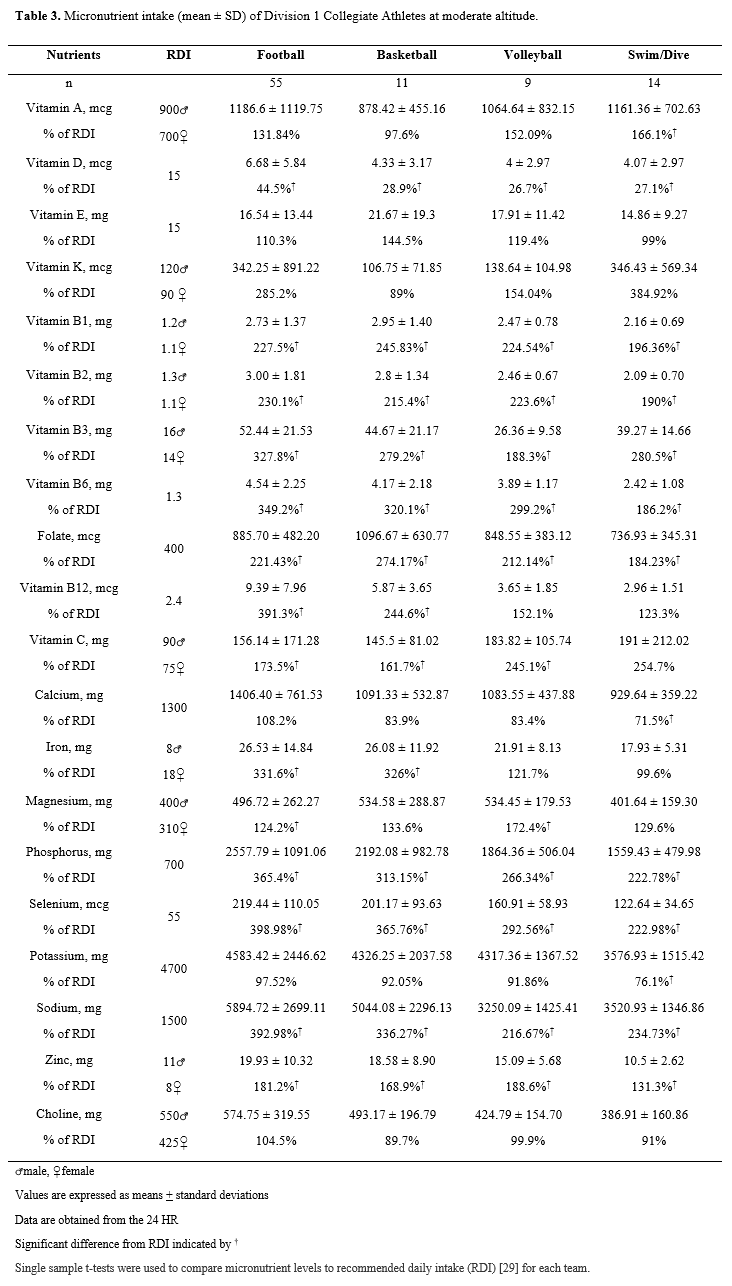
Table 3 indicates average micronutrient consumption by sport. Each team was significantly above the Reference Daily Intake (RDI) for many of the nutrients, but there were some exceptions, including Vitamin D (significantly below RDI for all teams), calcium (significantly below RDI for all teams except football), and potassium (significantly below RDI for swim/dive).
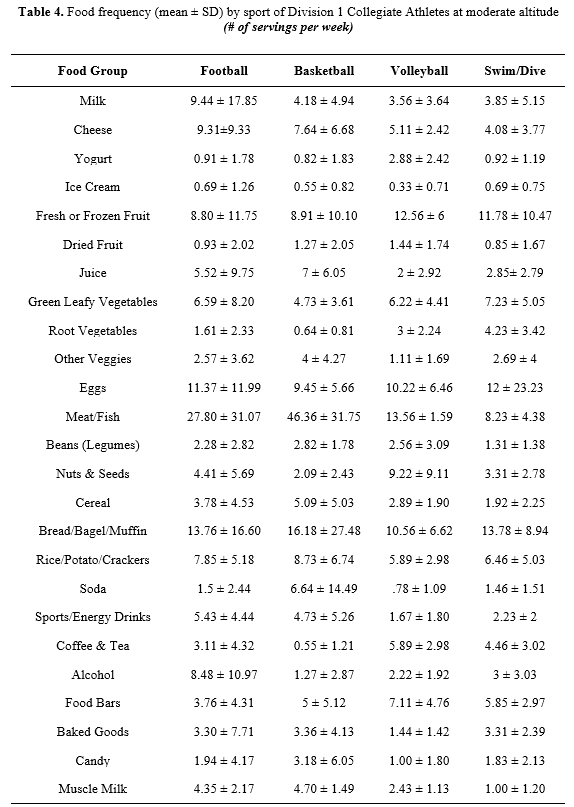
Descriptive results for the FFQ are presented in Table 4. From the results it is noted that there is great variability in dairy, alcohol, and juice consumption.
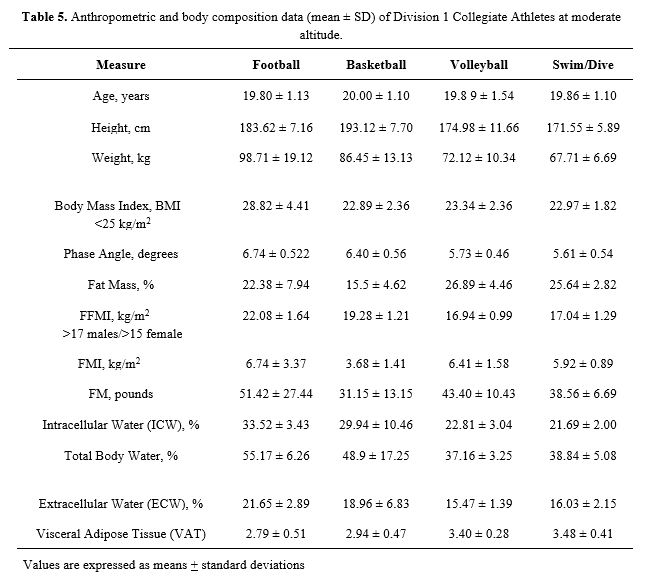
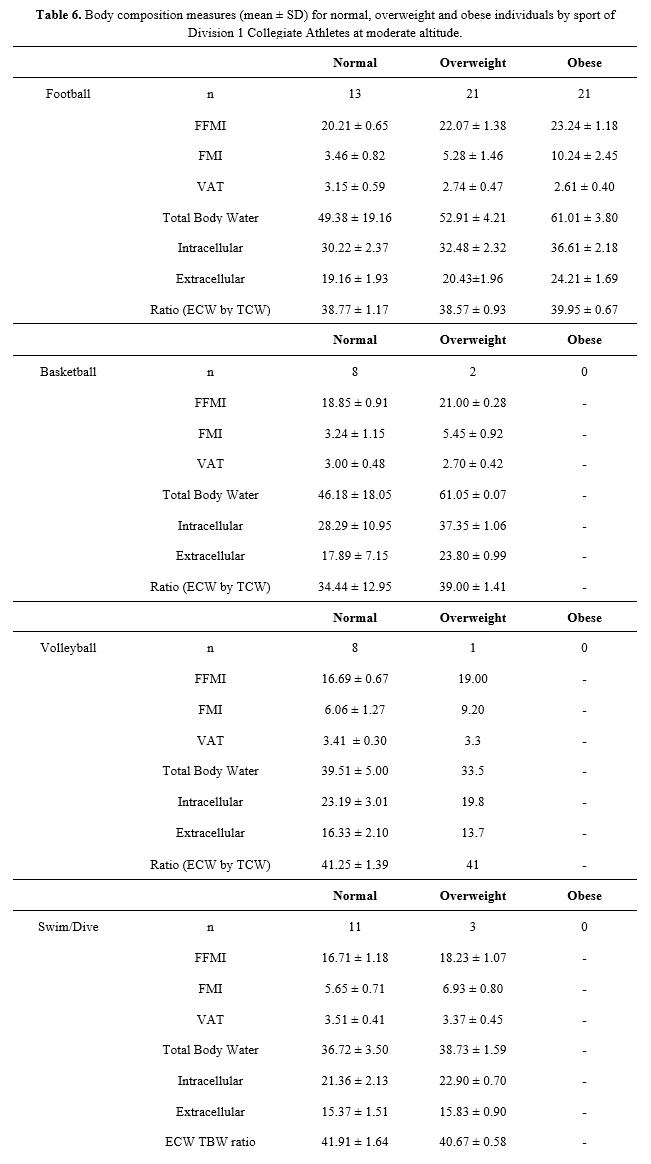
Anthropometric and body composition data measured by Seca® mBCA 515 are shown in Table 5. In this group of young healthy adults, we do not find too many health risks. BMI is higher than recommended for the football team but this may be related to increased muscle mass. Fat Free Mass Index (FFMI), Fat Mass Index (FMI), VAT and water measures in relationship to standard BMI categories are shown in Table 6. Football players in the obese category had a high FMI, but measures of VAT, TBW, ICW, ECW, and ECW/TBW ratios are in the normal range.
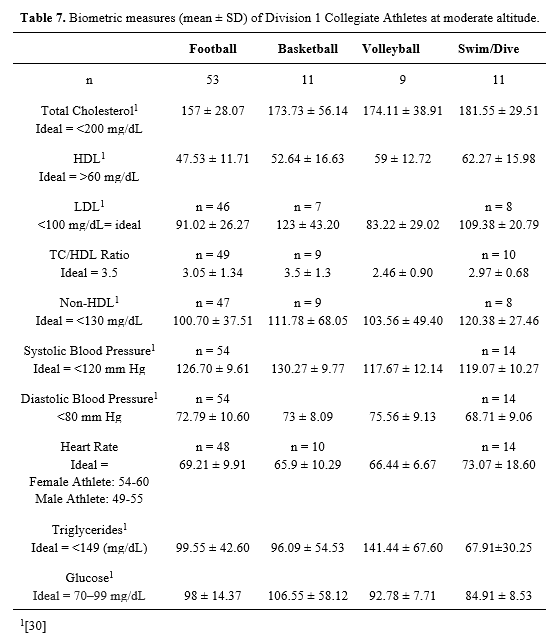
Biometric measures are shown in Table 7. Total serum cholesterol was at recommended levels for all teams. Low-density Lipoprotein (LDL) and Total Cholesterol/High-Density Lipoproteins (TC/HDL) ratios were at acceptable levels with the exception of men’s basketball, they were at borderline levels. Triglycerides and blood glucose were at the recommended levels for all athletes, except for men’s basketball, which showed greater-than-ideal fasting blood glucose levels. Resting heart rate and diastolic blood pressure were at recommended level for all teams, but systolic blood pressure was higher than recommended for the men’s teams. Although most team average values for body composition and biomarkers indicate that there are minimal health risks, there is significant variability in the data. It should also be noted that with the relatively small sample sizes, a single outlier can have a major impact on team measures.
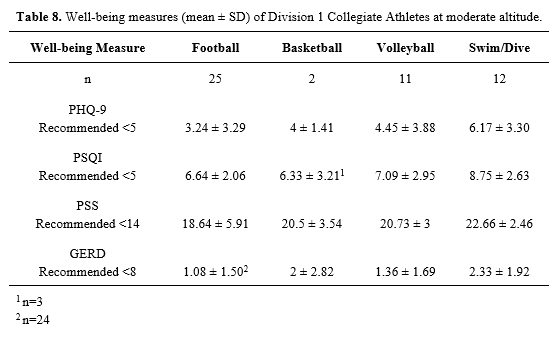
Wellness measures are shown in Table 8. For depressive symptoms only swim and dive scored above recommendation. Sleep quality and stress scores were above recommended levels for all teams. GERDQ scores were at recommended levels for all teams.
DISCUSSION
We found a trend of consistent under-consumption of energy across teams, which is likely to impact training, performance and optimal recovery (24). As energy expenditure of athletes at moderate altitude has been reported to be 2.5-3 times higher than athletes at sea level (28) this specific student-athlete population may have even greater caloric needs than currently assumed. Furthermore, exposure to moderate altitude has been shown to suppress hunger and appetite (28). One approach to addressing low energy availability at moderate altitude could be to encourage student-athletes to consume foods more frequently as well as more liquid foods that are potentially more tolerable when hunger is suppressed.
Carbohydrate and Dietary Fiber
As all participants were involved in 1-3 hours/day of moderate to high-intensity exercise most days, recommended carbohydrate intake was 6 – 10 grams per kilogram per day (g/kg/d) (7). No athlete group exceeded 4.61 g/kg/d. Demanding intermittent high-intensity movements over a prolonged period of time in all of these athletes could necessitate carbohydrate ingestion before, during, and after exercise (2). Additionally, adequate glycogen replenishment between training sessions should be emphasized in future educational efforts, since depletion of glycogen stores are associated with fatigue and a corresponding reduction in work rates, impaired skill and concentration, and increased perception of effort (37). Overall dietary fiber intake was at or over recommended amounts with the exception of football. Specific recommendations to improve carbohydrate and fiber consumption could include timing the intake of carbohydrates, consumption of nutrient-dense, low glycemic index carbohydrates sources, as well as the use of liquid sources of carbohydrate when appetite may not adequately stimulate the desire to eat.
Protein
Although all teams easily met their protein needs with food consumption alone, it is possible that a portion of the protein intake was siphoned away to meet energy needs at the expense of protein synthesis or maintenance. If total energy deficit were to continue, increasing protein intake > 2.0 g/kg/d should be considered (27). Of equal importance is the need for protein periodization to ensure that protein is consumed before and after exercise sessions and every 3 to 5 hours over multiple meals (35). The males tended to have more animal protein ingestion while the female athletes tended towards more diversity of blending animal and plant proteins. Higher plant-based protein sources lead to a corresponding increased consumption of micronutrients and should be encouraged in all athletes.
Dietary Fat
The male student-athletes in this study were found to be above the recommended levels for total and saturated fat and all student-athletes were found to be lacking in Omega-3 eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) fats.
The ability of EPA & DHA to potentially decrease inflammatory markers is of utmost importance to athletes and their overall training and performance (18). This information will guide our future educational efforts to ensure that athletes are aware of the food sources, such as seeds, nuts, leafy greens, and fatty fish that are rich in EPA, DHA and the related precursors.
Dietary Cholesterol
Since three of the four teams exceeded the daily dietary cholesterol recommendations, nutrition education efforts should be made to help these student-athletes adjust their food intake in an effort to minimize the potential increased risk of endothelial dysfunction, atherosclerosis, heart disease, and subsequently reduced blood flow needed for working muscles (13).
Alcohol
Athletes are often encouraged to abstain from alcohol to avoid the potentially detrimental effects on sports performance and recovery (4). Football reported they consumed on average 8.48 servings per week. Although this is consistent with the findings of others, it is significantly higher than the other sports teams reported (19). Student-athletes should consider abstinence or alcohol consumption with a calculated approach, whereby they stay within the reported dose of approximately 0.5 g/kg of body weight or less to reduce the likelihood of impacting recovery and sports performance (4).
Micronutrients
The micronutrient consumption reported in this study revealed tremendous variability. The micronutrients of specific importance for athletic performance include vitamin D, calcium, iron, the B-vitamins, choline, and magnesium. Of these, the only ones that showed deficiencies amongst the athletes were vitamin D and calcium. Vitamin D is important for calcium regulation and bone health; a chronic deficiency may lead to increased injuries and stress fractures. All athlete groups showed significant deficiencies of vitamin D consumption, which could be rectified by consuming Vitamin D-containing or fortified foods, and/or dietary supplementation. Calcium intake was suboptimal for three of the four teams. Calcium is vital for muscle contraction, bone mineralization, and blood circulation. As such, athletic training places additional demands on the body and calcium intake and absorption needs to be monitored.
Food Frequency Questionnaire
The food frequency patterns indicate tremendous variability and patterns among individuals, genders, and teams. There are multiple explanations for these differences, including individual and team culture, shared meals, and whether the participant lived on or off campus.
Anthropometrics and Body Composition
For all teams except football, FMI was in normal ranges for all participants. Of the 55 football players, 76.4 percent were classified as overweight or obese based on BMI. Within the overweight group of 21 individuals, all were classified within normal ranges of FMI. Within the obese group of 21 individuals, 71.4 percent had a high FMI. Those football student-athletes who were classified as obese are at increased risk for insulin resistance and metabolic syndrome. This is consistent with Borchers et al, who studied Division 1 collegiate football players and found that of the individuals who were obese (all linemen), 13 of 19 were insulin resistant, and all of them were living with metabolic syndrome (9). Borchers et al defined insulin resistance by using the Quantitative Insulin Sensitivity Check Index (QUICKI) calculations and metabolic syndrome using criteria from the NCEP ATP III clinical definition. It appears as though, those athletes that tend to store more body fat in the abdominal region, and have higher levels of VAT, may need additional education on how they can adopt lifestyle behaviors that will help minimize the cardiometabolic risks associated with increased VAT.
Hydration at moderate altitude is known to be an added concern for athletes. Participants in this study showed great variability in levels of hydration, as measured by Seca® mBCA 515. With the dry air at moderate altitude, the lungs must humidify the air, which may require additional fluids. In future education efforts, it is imperative to emphasize the need to monitor hydration status closely.
Biometrics
Since the mean age of the participants in this study was 19.84 years old and the average physical activity levels were high we did not anticipate widespread abnormalities in serum biometric factors. However, the total cholesterol, systolic blood pressure, and fasting blood glucose levels were slightly elevated with men’s basketball. A potential relationship may exist between these elevated readings and the number of processed foods and animal protein consumed. By providing all athletes with information and practical tips on how to consume more energy-dense as well as nutrient-dense food choices the overall dietary profile may improve in relation to also consuming more micronutrients.
Well-Being Measures
There was an overall less than desirable quality of sleep experienced across the teams. In addition, the swim/dive participants had the most unfavorable readings for all well-being measures, except GERD. One explanation might be that the swim/dive participants have a long competitive season that may contribute to an overall decrease in well-being.
CONCLUSIONS
In light of the findings of low energy availability in this assessment, we are now scheduled to conduct an investigation with the football student-athletes aimed at determining the primary causes of this low energy availability trend. We will be assessing: access to food, appetite, hunger, nutrition knowledge, and other factors associated with limited food consumption.
APPLICATIONS IN SPORT
Our study supports the notion that collegiate student-athletes would benefit by having either team nutrition education and/or individualized nutrition counseling available (30). There is a need for basic and practical food education that takes into consideration current guidelines and that emphasizes strategic food consumption e.g., meal timing, fluid timing, travel tips, season variability in training: in-season versus off-season plans, and tournaments. However, since dietary habits are ingrained in a complex interaction of multiple factors it is imperative to provide educational methods that allow for personalization (6, 34). In addition, overall wellness and implications of moderate altitude need adequate attention in future educational sessions. It is also important to include the coaching and support staff in all educational efforts.
ACKNOWLEDGMENTS
The authors would like to acknowledge the support of the Plant-Rich and Nutrient Dense Interventions for Active Lifestyles (PRANDIAL) Lab at Northern Arizona University as well as the individual athletes who participated in this research. Special mentions go toWendy Wetzel, Dierdra Bycura, Arron Shiffer, Sara Moore, and Anthony Santos for their help conducting the testing and Sam Lawson and Barbara-ann Herkens for their help with literature reviews. This research was funded by the Eric M. Lehrman 2015 Trust and Northern Arizona University Department of Health Sciences, 2018.
REFERENCES
- American Dietetic Association. (1996). Food Frequency Form. Medical Nutrition Therapy Across the Continuum of Care. American Dietetic Association: Chicago, Illinois, USA.
- Baker, L.B., Rollo, I., Stein, K.W., & Jeukendrup, A. E. (2015). Acute effects of carbohydrate supplementation on intermittent sports performance. Nutrients, 7(7), 5733-63. doi: 10.3390/nu7075249.
- Baranauskas, M., Stukas, R., Tubelis, L., Žagminas, K., Šurkienė, G., Švedas, E.,… Abaravičius, J.A. (2015). Nutritional habits among high-performance endurance athletes. Medicina, 51(6), 351-362. doi: https://doi.org/10.1016/j.medici.2015.11.004
- Barnes, M.J. (2014). Alcohol: impact on sports performance and recovery in male athletes. Sports Medicine, 44, 909-19. doi: 10.1007/s40279-014-0192-8
- Borchers, J., Clem, K., Habash, D., Nagaraja, H., Stokely, L., & Best, T. (2009). Metabolic syndrome and insulin resistance in division 1 collegiate football players. Medicine and Science in Sports and Exercise, 41(12), 2105-2110. doi: 10.1249/MSS.0b013e3181abdfec
- Burke, L.M., Hawley, J.A., Wong, S.H.S., & Jeukendrup, A.E. (2011). Carbohydrates for training and competition. Journal of Sports Sciences, 29(1), S17-S27. doi: 10.1080/02640414.2011.585473
- Burke, L.M., Ross, M.L., Garvican‐Lewis, L.A., Welvaert, M., Heikura, I.A., Forbes, S.G.,… Hawley, J.A. (2017). Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers. Journal of Physiology, 595(9), 2785–2807. doi: 10.1113/JP273230
- Buysse, D.J., Reynolds, C.F., Monk, T.H., Berman, S.R., & Kupfer, D.J. (1989). The Pittsburgh Sleep Quality Index (PSQI): A new instrument for psychiatric research and practice. Psychiatry Research, 28(2), 193-213.
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385-396.
- Cole, C.R., Salvaterra, G.F., Davis, J.E. Jr, Borja, M.E., Powell, L.M., Dubbs, E.C., & Bordi, P.L. (2005). Evaluation of dietary practices of National Collegiate Athletic Association Division I football players. Journal of Strength and Conditioning Research, 19(3), 490-4. doi: 10.1519/14313.1
- Debevec, T. (2017). Hypoxia-related hormonal appetite modulation in humans during rest and exercise: Mini review. Frontiers in Physiology, 8(366), 1-8. doi: 10.3389/fphys.2017.00366
- Department of the Army. (2002). Military mountaineering (Field Manual No. 3-97.61). Washington, DC: U.S. Government Printing Office.
- Favero, G., Paganelli, C., Buffoli, B., Rodella, L.F., and Rezzani, R. (2014). Endothelium and its alterations in cardiovascular diseases: Life-style intervention. Biomedical Research International, 2014, 801896. doi: [10.1155/2014/801896]
- Harris, P.A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J.G. (2009). Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377-81. doi: [10.1016/j.jbi.2008.08.010]
- Institute of Medicine via National Academies of Sciences, Engineering, and Medicine. A complete document containing the four tables listed [at Dietary Reference Intakes Tables and Application: Health and Medicine Division, November 30, 2010].
- Jones, R., Junghard, O., Dent, J., Vakil, N., Halling, K., Wernersson, B., & Lind, T. (2009). Development of the GERDQ, a tool for the diagnosis and management of gastroesophageal reflux disease in primary care. Aliment Pharmacol Therapies, 30(10), 1030-8. doi: 10.1111/j.1365-2036.2009.04142.x
- Jonnalagadda, S.S., Rosenbloom, C.A., & Skinner, R. (2001). Dietary practices, attitudes, and physiological status of collegiate freshman football players. Journal of Strength and Conditioning Research,15(4), 507–513.
- Jouris, K. B., McDaniel, J. L., & Weiss, E. P. (2011). The effect of omega-3 fatty acid supplementation on the inflammatory response to eccentric strength exercise. Journal of Sports Science & Medicine, 10(3), 432–438.
- Kingsland, M., Wolfenden, L., Rowland, B.C., Gillham, K.E., Kennedy, V.J., Ramsden, R.L.,… Wiggers, J.H. (2013). Alcohol consumption and sport: a cross-sectional study of alcohol management practices associated with at-risk alcohol consumption at community football clubs. BMC Public Health, 13, 762. doi: 10.1186/1471-2458-13-762
- Kroenke, K., Spitzer, R.L., & Williams, J.B. (2001). The PHQ-9: validity of a brief depression severity measure. Journal of general internal medicine, 16(9), 606-613. doi: [10.1046/j.1525-1497.2001.016009606.x]
- Kumar, S., Dutt, A., Hemraj000000, S., Bhat, S., & Manipadybhima, B. (2012). Phase angle measurement in healthy human subjects through bio-impedance analysis. Iran Journal of Basic Medical Science, 15(6), 1180-4.
- Kushner, R. F. (1992). Bioelectrical impedance analysis: a review of principles and applications. Journal of the American College of Nutrition, 11(2), 199-209.
- Kyle, U. G., Sounder, E. P., Genton, L., & Pichard, C. (2012). Can phase angle determined by bioelectrical impedance analysis assess nutritional risk? A comparison between healthy and hospitalized subjects. Clinical Nutrition, 31(6), 875-881. https://doi.org/10.1016/j.clnu.2012.04.002
- Loucks, A. B., Kiens, B., & Wright, H. H. (2011). Energy availability in athletes. Journal of Sports Sciences, 29(S1), S7-15. doi: http://dx.doi.org/10.1080/02640414.2011.588958
- Lukaski, H. C. (2011). Micronutrient requirements for athletes. In B.I. Campbell & M. A. Spano (Eds.), NSCA’s Guide to Sport and Exercise Nutrition (pp. 90-108). Champaign, IL: Human Kinetics.
- Lukaski, H. C. (2004). Vitamin and mineral status: effects on physical performance. Nutrition, 20(7-8); 632- 644.
- Mettler, S., Mitchell, N, & Tipton, K.D. (2010). Increased protein intake reduces lean body mass loss during weight loss in athletes. Medicine & Science in Sports & Exercise, 42(2), 326-337. doi: 10.1249/MSS.0b013e3181b2ef8e
- Michalczyk, M., Czuba, M., Zydek, G., Zajac, A., & Langfort, J. (2016). Dietary recommendations for cyclists during altitude training. Nutrients, 8(6), 377. doi: 10.3390/nu8060377
- Moinuddin, S. (Northern Arizona University, Flagstaff, Arizona, USA). Personal communication, July 20, 2018.
- Nascimento, M., Silva, D., Ribeiro, S., Nunes, M., Almeida, M., & Mendes-Netto, R. (2016). Effect of a nutritional intervention in athlete’s body composition, eating behavior and nutritional knowledge: a comparison between adults and adolescents. Nutrients, 8(9), 535. doi: 10.3390/nu8090535
- National Heart, Lung, and Blood Institute. Retrieved from: https://www.nhlbi.nih.gov/files/docs/guidelines/atglance.pdf
- Norman, K., Stobäus, N., Pirlich, M., & Bosy-Westphal, A. (2012). Bioelectrical phase angle and impedance vector analysis – Clinical relevance and applicability of impedance parameters. Clinical Nutrition, 31(6), 854-861. https://doi.org/10.1016/j.clnu.2012.05.008
- Norman, K., Stobäus, N., Zocher, D., Bosy-Westphal, A., Szramek, A., Scheufele, R.,… Pirlich, M. (2010). Cutoff percentiles of bioelectrical phase angle predict functionality, quality of life, and mortality in patients with cancer. American Journal of Clinical Nutrition, 92(3), 612–19. https://doi.org/10.3945/ajcn.2010.29215
- Parks, R.B., Helwig, D., Deltmann, J., Taggart, T., Woodruff, B., Horsfall, K, & Brooks, M.A. (2016). Developing a performance nutrition curriculum for collegiate athletics. Journal of Nutrition Education and Behavior, 48(6), 419-424. doi: 10.1016/j.jneb.2016.03.002
- Phillips, S.M. (2014). A brief review of critical processes in exercise-induced muscular hypertrophy. Sports Medicing, 44(1), 71-77. doi: 10.1007/s40279-014-0152-3
- Sunami, A., Sasaki, K., Suzuki, Y., Oguma, N., Ishihara, J., Nakai, A.,… Kawano, Y. (2016). Validity of a semi-quantitative food frequency questionnaire for collegiate athletes. Journal of Epidemiology, 26(6), 284-291. doi: 10.2188/jea.JE20150104
- Thomas, D.T., Erdman, K.A., & Burke, L.M. (2016). Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. Journal of the Academy of Nutrition and Dietetics, 116(3), 501-528. doi: 10.1016/j.jand.2015.12.006
- United States Department of Agriculture Super Tracker. Retrieved from: https://www.supertracker.usda.gov/. \lsdlocked0 G
