Authors: Jessica M. Kerns, MSAT, LAT, ATC; Dani M. Moffit, PhD, LAT, ATC
Corresponding Author:
Jessica M. Kerns
Sport Science and Physical Education Department
219 S. 8th Avenue, Stop 8105
Pocatello, ID 83209-8105
208-996-6737
harrjes3@isu.edu
Cardiopulmonary Resuscitation and Automated External Defibrillator Certification of Club Coaches in Alaska, Idaho, Oregon, Montana, and Washington
ABSTRACT
Cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) qualifications for coaches within club sport systems appear largely unregulated. This is a concern because CPR/AED qualifications should be a safety consideration. This study attempted to identify the prevalence of CPR and AED certification for club sport coaches in five states, as well as assess the availability of AEDs at practices and games. Not all coaches surveyed identified having CPR (n=84, 72.6%) and/or AED (n=83, 75%) training. A majority of coaches reported having an AED at practice (n=43, 54.4%). For games, there were fewer coaches identifying the availability of an AED (n=36, 43.4%). While the majority of coaches report having CPR/AED certification several coaches did not select having both CPR and AED certification although AED is a part of all CPR training courses. There was no consistency as to the availability of an AED at practices or games. Through investigating this topic, it was learned that there is no overarching governing body in club sports and therefore, few agreed upon regulations.
Keywords: CPR; AED; club sports, qualifications, interscholastic
INTRODUCTION
Annually, 7.8 million student-athletes participate in interscholastic sports (8). With club sports becoming an all-consuming movement among parents, coaches, and athletes across the nation (4), many athletes choose to participate in club sports to specialize in hopes of gaining expertise to earn a scholarship for college athletics (13). Often, club sport organizations hire coaches who are either past players or assistant coaches from the surrounding area. There are also situations in which parents are needed to coach younger teams. This creates a conflict of interest because often it is the outside sources (i.e., coach, parents) that pressure the athlete to pick a single sport in hopes of earning a college scholarship (13).
The underlying perception of specialization in club sports and practicing as many hours as possible may have arose from the concept that 10,000 hours of practice is needed in order to achieve a high level of performance (10). Even though some evidence supports the specialization in a single sport can help an athlete excel, it can also cause increased risk for dropout, physical risk, psychological harm, and social harm (1). This can be dangerous because most club sports practice multiple days a week in various facilities that may or may not have the proper emergency equipment in case an athlete is injured.
Additionally, coaches in many club sport organizations are not always affiliated with interscholastic athletics, which creates a gap in training procedures. Not having an affiliation with the schools allows for flexibility with the practice hours, how many games are scheduled, or where practices and games are to be held during the week (13). In addition to the aforementioned flexibility, it appears that requirements for training and education of coaches are managed by each individual club sport or organization/league, often not to the stringent guidelines of interscholastic athletics. This can be dangerous for the athletes who are left in the care of their coaches.
Within sport there is an inherent risk of injuries. These injuries can be acute (e.g. sprained ankle), chronic (e.g. Little League elbow), season ending (e.g. ruptured ACL), or in some cases, catastrophic (e.g. severed spinal cord; 3). Sudden cardiac arrest (SCA) is one of the leading causes of death amongst athletes during exercise (2) so exercise can become a risk factor for athletes with either diagnosed or undiagnosed cardiovascular disorders (7).
Commotio cordis, one cause of SCA, occurs when an athlete receives as a blunt, non-penetrating trauma to the chest causing an irregular heart rhythm, frequently resulting in death (9). Approximately 50 percent of commotio cordis events are reported in the sports of baseball, softball, ice hockey, football, or lacrosse in which athletes may receive a blow to the chest by a ball, puck, or stick (7). Even though comotio cordis is just one example of SCA, research demonstrates other types of SCA events can occur with young athletes. In a two-year prospective study that included 2149 schools, a total of 129 high schools reported an SCA event. In these high schools, 26 cases were confirmed SCA events, 18 of which involved athletes, 13 happened outside the school campus, and four of the cases were provoked by a head trauma (6). Survival rate of an SCA event can be as low as fifteen percent due to the lack of early recognition and failure to start resuscitation (7).
Even though the survival rate from SCA is low, an emergency action plan including quick response for CPR and use of an AED within three minutes will increase the athlete’s chance of survival (7). Since most SCA incidents happen during sporting events, location of AEDs at facilities should be carefully considered (11) with it being suggested that AED units be placed in a secure area that can be unlocked and available during both practices and games (11). However, if coaches aren’t trained in CPR or the use of AEDs, having the AED available may be futile. Therefore, the purpose of this study is two-fold: to identify the prevalence of CPR and AED certification for club sport coaches in five states, and to assess the availability of AEDs at practices and games.
METHODS
Participants
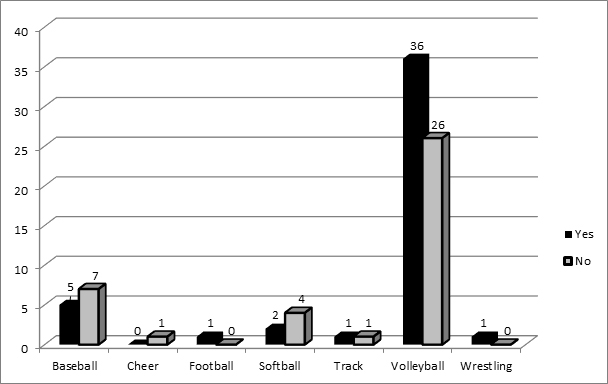
Participants were from the National Athletic Trainers’ Association (NATA) District 10 states (Alaska n = 12, Idaho n = 11, Oregon n = 15, Montana n = 6, and Washington n = 39) who coach youth club sports of volleyball, softball, and baseball. A total of 86 club coaches responded to the survey, with number of coaches responding by sport in Figure 1.
Figure 1. Number of coaches responding by sport
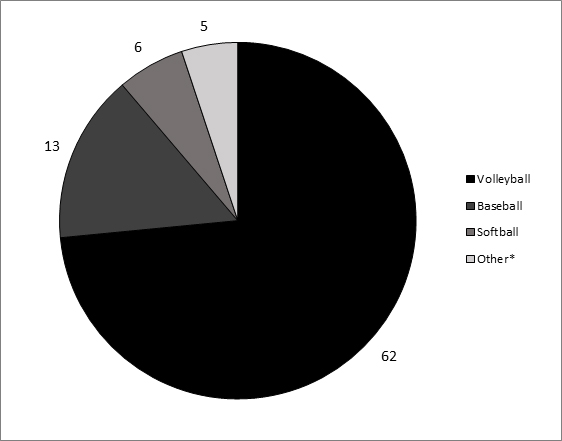
*Some coaches indicated they coached multiple club sports (e.g., baseball, cheerleading, football, track, wrestling)
Procedures
Once the university institutional review board approved this study, participants were contacted through an email that gave information on the purpose of the study, a confidentiality statement, and a link to the survey on SurveyMonkey. By selecting the link, consent was given to participate. Contact information for each club sport’s coach was obtained through web searches on each states club sports websites, along with phones calls to club directors or board members. The online survey consisted of demographic information (e.g., sport coached, age group coached, gender coached, state, and position held) and sections regarding: 1) certifications the coach possesses, 2) the distance an AED is from practice, and 3) the distance an AED is from game events.
Statistical Analysis
Descriptive statistics (frequencies and percentages) described prevalence of CPR and AED certification. Variables included: sport, state, practice, games, CPR certification, AED certification, and time to retrieve AED unit. Pearson’s product moment correlation was used to analyze relationships between CPR/AED certifications by state and sport, use of cardiac tools used, and AED availability at practice and games. Alpha was set at p<0.05.
RESULTS
Sixty-two (72.6%) coaches reported having CPR certification and 45 (52.3%) reported having AED certification. Coaches CPR certification status by state is found in Figure 2. Of the 68 ‘yes’ responses to the CPR certification, 30 (44%) were from Washington. Figure 3 describes AED certification by state, with the highest proportion coming from Washington. Figures 4 and 5 show CPR and AED certification, respectively, by sport.
Figure 2. Number of CPR certified coaches by state
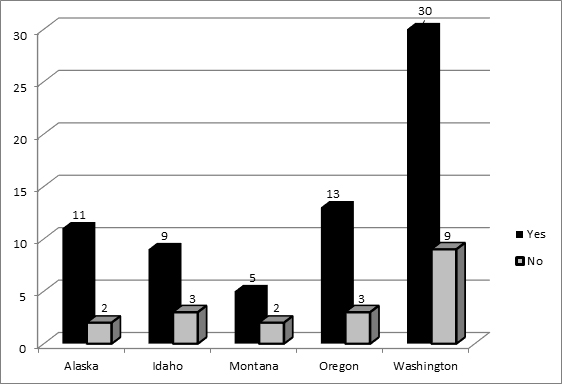
Figure 3. Number of AED certified coaches by state
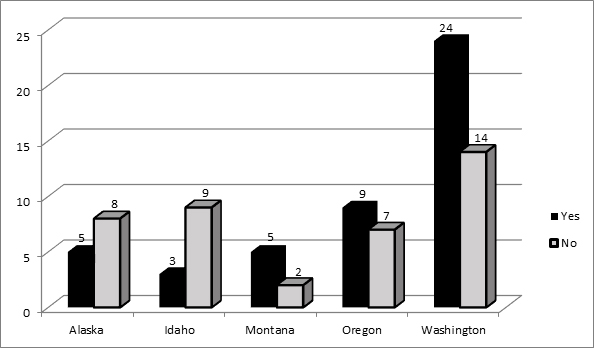
Figure 4. Number of CPR certified coaches by sport
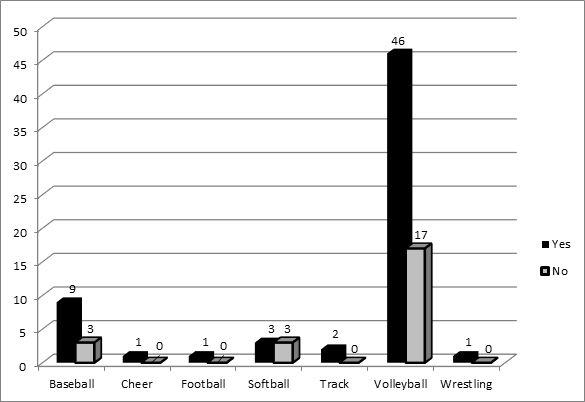
Figure 5. Number of AED certified coaches by sport
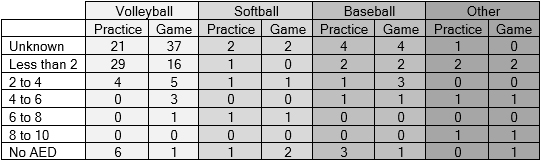
Two to four minutes was the most common response when asked how far away an AED is from the practice facility (Table 1). When asked how far away an AED is from a game, the most common response was unknown (Table 1).
Table 1. Perceived time (in minutes) to AED during practice and games.
DISCUSSION
There is a paucity of research examining CPR/AED certification for coaches and AED availability in regard to club sports. It was hypothesized that coaches of club sports would have training in CPR/AED to equivalent interscholastic coaches. Additionally, AEDs would be readily available at practices and games. However, the results obtained do not support either hypotheses.
Certification in CPR and AED for coaches is not common in public schools, which is concerning since many schools do not have athletic trainers (5). This lack of uniformity often means that responsibility and the liability of treatment provided for athletes falls on undertrained coaches, rather than on trained professionals (e.g., athletic trainers), who have been properly educated (2). In cases where athletic trainers are not available, first-line personnel should be educated in recognition of cardiac emergencies, certified in the use of CPR and AED, and know the location of the AED (11). NATA strongly suggests coaches have training in CPR, AED, and first aid to ensure they can deliver treatment to the athlete until medical professionals arrive (2). Results from the current study revealed that coaches indicated having either CPR or AED certification, but not always both. This conflicts with all CPR courses, as AED training is included in the course. This seems to indicate that more emphasis is placed on resuscitation rather than use of AED units in an emergency situation.
Financial concerns are cited as one of the main reasons for lack of AED units on and off school campuses (5). Two-thirds of SCA events happen at sporting events and so priority should be placed on expanding AED locations on campuses where sporting events happen (6). One concern is that an AED available inside the building will not be helpful while on an outdoor field; personnel may not always transport AEDs to an outdoor field of play.
Placement of AED units in public locations for access and use by either trained or untrained personnel has improved survival rates of out-of-hospital cardiac arrest (12). Early defibrillation has been demonstrated as the greatest contribution to survival following out-of-hospital cardiac arrest with survival rates decreasing seven percent to ten percent with every minute that defibrillation is postponed (12). New programs have been implemented to educate typical first responders and non-traditional first responders in CPR and AED use to help with the early defibrillation at sporting events (6). Survival from out-of-hospital SCA doubled when typical first responders and non-traditional survivors were trained in CPR and AED use, including AED use as part of an emergency action plan or some sort of practiced response for shorter response times (6). The current study found that there is no consistency concerning the availability of AEDs at practices and games. Location of practice and games (indoor vs. outdoor) did not affect results.
There are several limitations to this study. The survey was sent out through email and social media, so it is unknown how many coaches received the survey due to old email addresses, individuals no longer coaching, or email address errors. The sample size of coaches was adequate but the return rate of surveys was marginal. Club sports are individual organizations in nature with little apparent communication between clubs. There did not appear to be a central point of access to distribute communications and most club administrators did not want to give out personal emails. Information was sent about the study with the link for the survey to the club administrators but the researchers had no way of knowing whether the administrators passed on the information to their coaches.
CONCLUSIONS
The current research describes the qualification requirements that may be lacking with club sport coaches. Future research should examine how coaches are educated in CPR and AED use in both the interscholastic and club sport settings. Research should also look at the benefits of CPR/AED certification and AED availability in club sports in relationship to cost and the potential cost risks of not doing so.
APPLICATIONS IN SPORT
One of the major challenges is convincing individual governing bodies in club sports to recognize that cost associated with CPR and AED certification may reduce the overall cost associated with potential litigation for not doing so. Club sport organizations should not only be concerned with enhancing athletes’ abilities, but also make sure athletes can succeed in their sport with minimal injuries. By standardizing the certifications club coaches must possess, as well as making sure the proper safety equipment is available (i.e., AED), better protection of the athletes can be fostered. Parents of these athletes expect the coaches to be the best; they should also expect the protection for their athletes to be at a high standard, as well.
ACKNOWLEDGMENTS
None
REFERENCES
1. Baker, J., Colby, S., & Fraser-Thomas, J. (2009). What do we know about early sport specialization? Not much! High Ability Studies, 20(1):77-89. doi: 10.1080/13598130902860507
2. Casa, D. J., Guskiewicz, K. M., Anderson, S. A., Courson, R. W., Heck, J. F., Jimenez, C. C., …Walsh, K. M. (2012). National athletic trainers’ association position statement: Preventing sudden death in sports. Journal of Athletic Training, 47(1):96-118. Retrieved from http://natajournals.org/loi/attr
3. Cassas, K, & Cassetari-Wayhs, A. (2006). Childhood and adolescent sports-related overuse injuries. American Family Physician, 73(6): 1014-1022. Retrieved from http://www.aafp.org/journals/afp.html
4. Christianson, P., & Deutsch, J. (2012) Making a case for early sport specialization in youth athletes. Journal of Youth Sports, 6(2): 3-6. Retrieved from http://jss.sagepub.com/content/35/3/306.short
5. Dewitt, T., Unruh, S., & Seshardri, S. (2012). The level of medical services and secondary school-aged athletes. Journal of Athletic Training, 47(1): 91-95. Retrieved from http://natajournals.org/loi/attr
6. Drezner, J., Toresdahl, B., Rao, A., Huszti, E., & Harmon, K. (2013). Outcomes from sudden cardiac arrest in US high schools; a 2-year prospective study from the National Registry for AED use in sports. British Journal of Sports Medicine, 47: 1179-1183. doi: 10.1136/bjsports-2013-092786
7. Halabchi, F., Seif-Barghi, T., & Mazaheri, R. (2011). Sudden cardiac death in young athletes; A literature review and special consideration in Asia. Asian Journal of Sports Medicine, 2(1): 1-15. Retrieved from http://asjsm.com/
8. High school participation increases for 25th consecutive year. National Federation of State High School Associations. https://www.nfhs.org/articles/high-school- participation-increases-for-25th-consecutive-year/. Published October 30, 2014. Accessed March 4, 2016.
9. Palacio, L., & Link, M. (2009). Commotio cordis. Sports Health, 1(2): 174-179. doi: 10.1177/1941738108330972
10. Smith, M. (2015). Early sport specialization: A historical perspective. Kinesiology Review, 4(3): 220-229. Retrieved from http://www.americankinesiology.org/kinesiology-review
11. Toresdahl, B., Courson, R., Borjesson, M., Sharma, S., & Drezner, J. (2015). Emergency cardiac care in the athletic setting: From schools to the Olympics. British Journal of Sports Medicine, 46(Suppl I): 85-89. doi: 10.1136/bjsports-2012-091447
12. Wasilko, S., & Lisle, D. (2103). Automated external defibrillators and emergency planning for sudden cardiac arrest in Vermont high school: A rural state’s perspective. Sports Health, 5(6): 548-552. doi: 10.1177/1941738113484250
13. Watts, J. (2002). Perspectives on sport specialization. Journal of Physical Education, Recreation & Dance, 73(8): 32-37, doi:10.1080/07303084.2002.10608327
