Authors:
Elizabeth K. Wells, Exercise Science Department, Campbell University, Buies Creek, NC, USA
Megan L. Avery, Valencell Inc., Exercise Science Department, Campbell University, Buies Creek, NC, USA
L. Chris Eschbach, Valencell Inc., Raleigh, NC 27609
Jennifer Bunn, Department of Physical Therapy, Campbell University, Buies Creek, NC, USA
Corresponding author:
Jennifer Bunn
Campbell University, Department of Physical Therapy
4250 US 421 South
Lillington, NC 27546
910-893-1361
bunnj@campbell.edu
A Comparison of Perceived Physical Fitness and Objective Measurements
ABSTRACT
The purpose of this study sought to analyze the contribution of perceived physical fitness compared to one’s actual level of fitness. In this study, participants subjectively assessed their own cardiovascular fitness (CVF; n = 85) and body composition (BC; n = 110) on a scale of one (poor) to ten (excellent). The participants then underwent body composition testing, via 7-site skinfold, and completed a maximal graded exercise test on either a treadmill or cycle ergometer. Data from the exercise and body composition tests were compared to normative data to determine their percentile rank. Cohen’s Kappa Statistic was used to determine congruence between the predicted and observed CVF and BC values. Results indicated that the participants’ perceived BC had poor agreement (κ < 0.20), and perceived CVF had no agreement (κ < 0), when compared to actual measurements taken. These results suggest that an individual’s perception of their CVF and BC were not accurate. Similarly to how participants will provide inaccurate reports of diet and physical activity, these individuals are likely to have an inaccurate report of their fitness level. While most research suggests these discrepancies are due to pressures from society and a desire to conform, other research demonstrates that society is uneducated and unable to report an accurate fitness level.
Keywords: body composition, cardiovascular fitness, maximal oxygen consumption, fitness
INTRODUCTION
An individual’s perception of fitness is constructed by physiological experiences and psychological feelings. Individuals often subject themselves to psychological stressors and sociocultural pressures, such as lower self-esteem, unintentionally. Such stressors can contribute to creating inaccuracies and misconceptions in their actual quantified and perceived parameters of health, cardiovascular fitness (CVF) capabilities as measured by oxygen consumption (VO2), body composition (BC), dietary intake, and physical activity. Some research suggests that social desire affects most individuals to a certain degree, indicating that individuals become displeased with their health or look, and today’s media exposure often portrays artificial and unattainable physiques (6, 24).
Many factors contribute to an obsession with dieting (15) and could be driving individuals to falsely report their food intake or exaggerate their physical activity, BC, and CVF levels when self-reporting dietary and fitness assessments. Vancampfort et al. (25) found that a group of participants with eating disorders improved their perceived body image and self-esteem within six months after beginning an exercise regimen and healthy diet. Each participant reported having a higher and better fitness level even if their test results did not coincide with their perception. This leads to speculation that confidence could also play a role in fitness perception. Participants who felt overconfident about their fitness were more likely to report a fitness level that is higher than their actual fitness, and those who are less confident tend to report lower fitness levels.
Social desirability has also been described as one of the most common sources of bias affecting the validity of experimental and survey results (20). This emphasis on social desirability (diet, body image, health) presents as a major obstacle for individuals to conform to societal norms. Studies have shown that 46% of subjects admitted to intentionally under-reporting portion sizes, altering eating patterns, or omitting foods from their dietary intake records (3, 18). Another study proposed that most subjects report dietary intakes close to their perceived cultural or population norms rather than to their actual intake, which most likely arises from the influences of social desirability, social/peer pressure, and social attitudes towards food behaviors (23).
Similarly to inaccurate accounts of dietary intake, falsely reporting physical activity is likely related to the individuals’ wish to present their self in a positive light by giving a socially desirable response, describing themselves in favorable terms (21). Physical activity demonstrates a variety of factors that are all more subject to over-reporting (duration, frequency, intensity), which directly affects perceived CVF (8). Studies suggest that less educated and older males may have a predisposition to over-report physical activity from past athletic experience, whereas younger and higher educated males are more likely to under-report (1). Additionally, an escalating number of studies have directly assessed populations that are more likely to falsely report dietary intake, physical activity, CVF, and BC. Some false reports may be due to a lack of access to tools that assist with assessing their own physical condition in an objective, accurate manner (27). However, many studies have discovered that false reporting is typically more frequent among dissatisfied women and in overweight or obese individuals, which is most likely because these groups are less happy with their body shape and diet (4, 7, 9). According to a study done by Jeong (13), women, especially college women, tend to show a higher degree of somatotype distortion compared to that of their male counterparts. Additionally, when asked to determine physical fitness, participants tend to rely on only body weight to determine their physical fitness. If the participant felt overweight or underweight, it was reported as poor fitness (1, 8, 16). However, body weight is not a sole determinate of physical fitness. Therefore, some participants were likely to have given inaccurate reports based on weight. Overall, the legitimacy of self-reports is affected by the underreporting of socially undesirable characteristics and the over reporting of socially desirable behavior.
Previous studies conclude that self-reported exercise is especially vulnerable to participant bias based on societal pressures and media (6, 15), social desirability (3, 19, 21, 23), prior physical fitness (5, 8, 12, 16), and BC (1, 8, 16), which can all affect a person’s perceived physical fitness. The purpose of this study was to compare perceived physical fitness with objectively measured CVF and BC.
METHODS
Participants
This study consisted of participants that contacted the Human Performance Lab at Meredith College to seek an evaluation of either their CVF or BC. All 110 participants completed BC testing (males, n = 57; females, n = 53). However, of these participants, 85 (males, n =44; females, n =41) participants completed the CVF testing. Thus, the two data sets were analyzed separately with 110 participants used for CVF analyses and 85 participants used for BC analyses. Before testing procedures, all participants read and signed university-approved documents. Once the paper work was completed, the participants were asked to quantify their perceived levels of CVF and BC from zero (well below average) to ten (well above average) as it related to the general population.
Protocol
For CVF testing, participants performed a maximal graded treadmill test. The individualized running speed was constant throughout the test while the grade was increased by 2% every two minutes. Participants completed the exercise test until volitional exhaustion. Oxygen and carbon dioxide were measured via a metabolic analyzer (Vacu-Med Mini CPX, Ventura, CA) during the test to assess VO2max heart rate, blood pressure, blood lactate, and rate of perceived exertion during the exercise test.
BC was completed using the 7-site skinfold technique (11). The seven sites utilized were the triceps, subscapular area, mid-axillary area, chest, abdomen, suprailiac, and thigh. Each site was measured three times and the mean of the three assessments was used to calculate body density and percent body fat. All BC measurements were completed by the same technician to avoid any bias.
CVF and BC values were ranked based on percentile values provided by the Institute of Aerobics Research and the Aerobic Center Longitudinal Study as published in the ACSM’s Guidelines for Exercise Testing and Prescription (2, 17, 22). Both CVF and BC gender-specific data are ranked and were used as normative data for comparison. For example, a 25 year-old female testing at 43 ml/kg/min for VO2peak would be categorized in the 70th percentile, and therefore given a rating of 7 for her actual CVF score. These ranked scores were compared to the perceived score given by each participant for their own CVF and BC.
Statistical Analyses
All statistical analyses were completed using IBM SPSS Statistics Data Editor 19 (Armonk, NY). Means and standard deviations were calculated for perceived rankings and for actual CVF and BC laboratory findings and percentile rankings. Significant differences between the predicted and observed CVF and BC values were tested using the Cohen’s Kappa Statistic. An alpha level of 0.05 was used to determine significance.
RESULTS
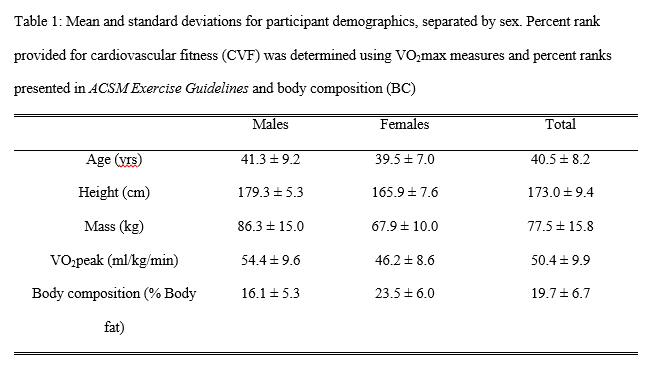
Table 1 displays participant demographics and the results from the CVF and BC laboratory tests. On average the participants in the study were younger middle-aged adults, with above average measures in both CVF and BC. Based on VO2max and BC assessments, these values were ranked according to standard norms (2, 17). Figure 1 shows the comparison between participant perceptions and measured values as broken down by sex.
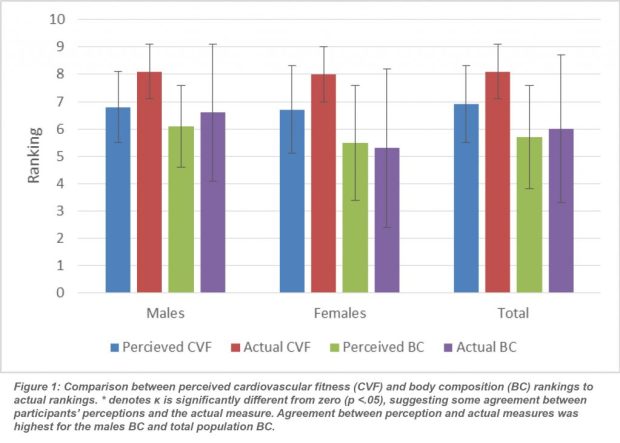
The Cohens Kappa test statistic was interpreted to indicate agreement between the participant perception and the actual measured values of CVF and BC (26). The results showed no agreement between the CVF perceptions and measures for males (κ =-.029) and the total population (κ =-.032), and slight agreement for the females (κ =.014). The BC results indicate that the participants’ predictions of their perceived BC had poor agreement for males (κ =.133), females (κ =.094), and the total population (κ =.094). The κ value was significantly different from zero for the males BC comparison (p =.002) and for the total population (p =.003). This suggests that the males tended to be more accurate in their BC perceptions, but the agreement was still poor. Perceptions of CVF showed no agreement (κ <0, p >.05) when compared to laboratory measurements taken. Both sexes showed poor perception of their actual CVF.
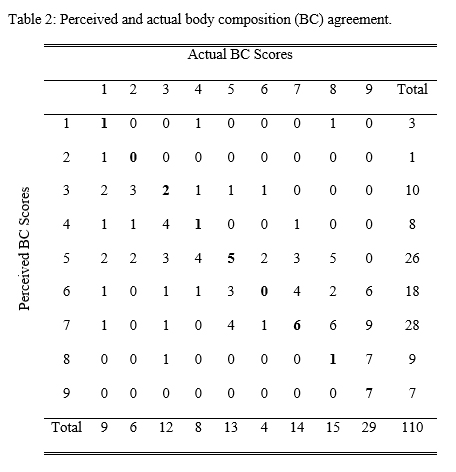
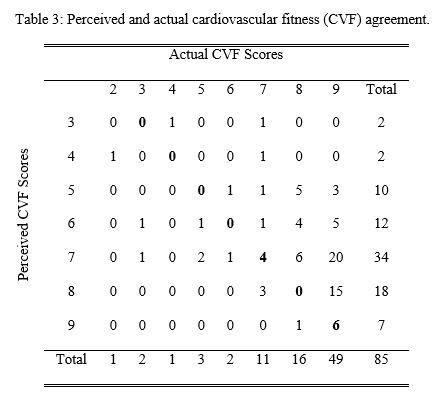
Tables 2 and 3 indicate the agreement of perceived and actual values for BC and CVF, respectively. Notably, both tables indicate that the subjects’ perceptions of themselves tended to gravitate towards the mean with higher predictions seen in the 5-8 range, whereas the laboratory measurements showed many subjects were found to be more evenly distributed.
DISCUSSION
This study sought to assess the accuracy in evaluating one’s own CVF and BC, and found there was little to no agreement with the actual measures. Psychological factors such as altered emotional states, body image, social desire, and self-worth affect the validity of participant’s perception. Intentionally or unintentionally, this affects the legitimacy of experimental and self-reports, which results in the underreporting or over reporting of diet and fitness.
The findings of this study showed that the participants tended to under-rank their CVF capabilities, men tended to slightly under-rank their BC, and women tended to slightly over-rank their BC; all resulting in little to no agreement between perceived and actual rankings. The participants’ perception of themselves tended to gravitate toward the mean, although the participants’ measurements were evenly distributed. Essentially, the majority of subjects gauged their fitness levels to be in the 50th to 80th percentiles. However, the actual measurements for the majority of participants were above the 70th percentile, and several were found to be below the 50th percentile. This is likely due to participants trying to place themselves in their idea of what is considered average or fit as seen in previous studies (6, 10, 15). In this study, BC in males tended to have the highest agreement, suggesting that the males tended to have greater accuracy in assessing their own BC. A previous study by Kagawa et al. (14) showed that difficulty in assessing BC generally exists because perceived “fatness” is generally associated relative to height and body shape. Subjects may have been overweight by body fat but did not consider themselves as so because their frame size was desirable.
Similar studies concur that individuals have the tendency to report themselves in socially favorable responses (15, 20, 21). The most notable inaccurate reporting that occurs in individuals are physical activity and dietary intake, which may have been based on acceptable norms rather than actual intake. Perceived fitness then becomes skewed because of the inaccurate reporting and can inhibit any further weight control or fitness progress (9). A study evaluating the association between self-reported physical fitness and performance-based measureS of physical fitness in overweight women found that self-reports should not be used as a substitute for performance-based tests (11). Women who over-reported their exercise showed poorer weight loss compared with those who accurately reported exercise. The authors concluded the participants that were over-reporting exercise were rating themselves based on fitness and diet goals that they wanted to achieve. This may be a likely reason the female data in this study showed an over-ranking of their BC because their CVF was so high, indicating they have high exercise participation.
There are clinical instances in which self-perceived fitness is as the sole assessment of one’s exercise participation and fitness capabilities. However, there are few studies that support this method as valid and reliable. Self-perceived fitness could be used in clinics to replace testing and also for personal gain for those without testing equipment that wish to improve fitness. Specifically, the participants in this study would be considered younger, middle-aged adults; therefore their perceived fitness could also be a predictor of risk related to heart disease and other chronic diseases. Blair et al. (2) completed a study on men that determined mortality risk based on an initial fitness and health evaluation and follow up evaluation. Men who improved their fitness and health from the initial evaluation had a less likelihood of dying from cardiovascular disease and all-cause mortality. The poor relationship between perceived fitness and actual fitness level for this age group of participants portrays the need for fitness testing available to middle-aged and older adults.
CONCLUSIONS
This study, along with past literature (15, 20, 21), supports that perception of fitness is not an accurate measure of an individual’s actual fitness. More studies should focus on this topic due to its importance in a clinical setting. Due to the rise in obesity and obesity-related health conditions, fitness perception and body composition are important to overall health. Adults rarely complete fitness testing or body composition testing, which means they have little feedback on their actual fitness level. A high waist circumference, body mass index (BMI), and percent body fat are among the health factors that predispose the development of heart disease, especially in middle aged adults. Furthermore, many sedentary or overweight individuals that are at risk for cardiovascular disease do not participate in exercise or have an accurate view of their health. Perception of fitness is proven to be an inaccurate measure of an individual’s actual fitness level (15, 20, 21); therefore, adults should regularly be participating in fitness testing and body composition measurements. The increase of education on this topic along with providing simple testing procedures in gyms or hospitals could help to increase the frequency of fitness testing in adults. Additionally, inclusion of activity feedback using commercially available activity trackers could also be used to help improve accuracy in CVF and BC perceptions.
APPLICATIONS IN SPORT
The data from this study is useful for personal trainers, exercise physiologists, and clinicians alike because it indicates the disconnect that many people have between perception and reality for their own health and fitness. These data help to show that the influence of media (both social and traditional), peers, and activity all impact one’s perception of themselves, which in turn likely impacts behavior. We suggest that personal trainers, exercise physiologists, and clinicians centered on fitness should regularly ask their clients/patients about their perceived fitness and compare it to actual measures. This will help to educate the lay public about their health and hopefully improve their health.
ACKNOWLEDGEMENTS
Thanks to Robin Leathers, Tristan Alston, and Brooke Catanzarito for your assistance on this project.
REFERNECES
1. Bassett, D., Ainsworth, B., Swartz, A., O’Brien, W., & King, G. (2000). Validity of four motion sensors in measuring moderate intensity physical activity. Medicine and Science in Sports and Exercise, 32(9 Suppl), S471-80.
2. Blair, S., Kohl, H. 3., Barlow, C., Paffenbarger, R. J., Gibbons, L., & Macera, C. (1995). Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. Journal of the American Medical Association, 273(14), 1093-8.
3. Blundell, J., & MacDiarmid, J. (1997). Fat as a risk factor for overconsumption: satiation, satiety, and patterns of eating. Journal fo the American Dietetic Association, 97(7), S63-9.
4. Cash, T., Winstead, B., & Janda, L. (1986). The great American shape-up. Psychology Today, 4, 30-37.
5. Conway, J., Seale, J., Jacobs, D., Irwin, M., & Ainsworth, B. (2002). Comparison of energy expenditure estimates from doubly labeled water, a physical activity questionnaire, and physical activity records. American Journal of Clinical Nutrition, 75(3), 519-25.
6. Fasting, K. (1986). Unemployment, trait anxiety and physical exercise. Scandinavian Journal of Sport Science, 8, 99-103.
7. Frederick, C., & Morrison, C. (1996). Social physique anxiety: personality constructs, motivations, exercise attitudes, and behaviors. Perceptual and Motor Skills, 82, 963-72.
8. Freedson, P., Melanson, E., & Sirard, J. (1998). Calibration of the Computer Science and Applications, Inc. accelerometer. Medicine and Science in Sports and Exercise, 30(5), 777-81.
9. Gray, S. (1977). Social aspects of body image: perception of normalcy of weight and affect of college undergraduates. Perceptual and Motor Skills, 45, 1035-40.
10. Hallinan, C., Pierce, E., Evans, J., DeGrenier, J., & Andres, F. (1991). Perceptions of current and ideal body shape of athletes and nonathletes. Perceptual Motor Skills, 72(1), 123-30.
11. Jackson, A., & Pollock, M. (1978). Generalized equations for predicting body density of men. British Journal of Nutrition, 40(3), 497-504.
12. Jakicic, J., Polley, B., & Wing, R. (1998). Accuracy of self-reported exercise and the relationship with weight loss in overweight women. Medicine and Science in Sport and Exercise, 30(4), 634-8.
13. Jeong, S.-J., & Chu, M.-S. (2010). The effects of somatotype and body image on apparel fashion orientation. Fashion & Textile Research Journal, 12(6), 764-773.
14. Kagawa, M., Kuroiwa, C., Uenishi, K., Mori, M., Dhaliwal, S., Hills, A., & Binns, C. (2007). A comparison of body perceptions in relation to measured body composition in young Japanese males and females. Body Image, 4(4), 372-80.
15. Khan, A. N., Khalid, S., Khan, H. I., & Jabeen, M. (2011). Impact of today’s media on university stuent’s body image in Pakistan: a conservative, developing country’s perspective. BMC Public Health, 11, 379.
16. Lichtman, S., Pisarska, K., Berman, E., Pestone, M., Dowling, H., Offenbacher, E., . . . Heymsfield, S. (1992). Discrepancy between self-reported and actual caloric intake and exercise in obese subjects. New England Journal of Medicine, 327(27), 1893-8.
17. Lohman, T. (1982). Body composition methodology in sports medicine. Physician and Sportsmedicine, 10(12), 46-58.
18. Mela, D., & Aaron, J. (1997). Honest but invalid: What subjects say about recording their food intake. Journal of the American Dietetic Association, 97(7), 791-793.
19. Mulligan, K., & Butterfield, G. (1990). Discrepancies between energy intake and expenditure in physically active women. British Journal of Nutrition, 64(1), 23-26.
20. Nederhof, A. J. (1985). Methods of coping with social desirability bias: A review. Eurpean Journal of Social Psychology, 15(3), 263-280.
21. Pate, R., Pratt, M., Blair, S., Haskell, W., Macera, C., Bouchard, C., . . . Wilmore, J. (1995). Physical activity and public health: A recommendation from the Cemters for Disease Control and Prevention and the American College of Sports Medicine. The Journal of the American Medical Association, 273(5), 402-407.
22. Pescatello, L. (2014). ACSM’s guidelines for exercise testing and prescription (9th ed.). Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health.
23. Schoeller, D. (1990). How accurate is self-reported dietary energy intake? Nutrition Reviews, 48(10), 373-9.
24. Tiggeman, M. (2014). The status of media effects on body image research: Commentary on articles in the themed issue on body image and media. Media Psychology, 17(2), 127-133.
25. Vancampfort, D., Probst, M., Adriaens, A., Pieters, G., De Hert, M., Stubbs, A., & Vanderlinden, J. (2014). Changes in physical activity, physical fitness, self-perception and quality of life following a 6-month physical activity counseling and cognitive behavioral therapy program in outpatients with binge eating disorder. Psychiatry Research, 219(2), 361-366.
26. Viera, A., & Garrett, J. (2005). Understanding interobserver agreement: The kappa statistic. Family Medicine, 37(5), 360-3.
27. Willers, D., Tse, G., Allsworth, J., Rutledge, B., Kovnar, S., & Macones, G. (2007). Assessing physical fitness: A study by Heimmel et al. American Journal of Obstetrics & Gynecology, 196(6), 610-611.
