Authors: Mark Hecimovich*(1), PhD, ATR; Doug King, PhD(2); Ida Marais, PhD (3)
(1) Division of Athletic Training, University of Northern Iowa, 003C Human Performance Center, Cedar Falls, Iowa, United States of America, mark.hecimovich@uni.edu
(2) Sports Performance Research Institute New Zealand (SPRINZ) at AUT Millennium, Faculty of Health and Environmental Science, Auckland University of Technology, Auckland, New Zealand, doug.king@clear.net.nz
(3) University of Western Australia, Graduate School of Education, M428, 35 Stirling Highway, Mount Crawley, Western Australia, ida.marais@uwa.edu.au
*Corresponding Author:
Mark Hecimovich, PhD, ATC
Division of Athletic Training, University of Northern Iowa, 003C Human Performance Center, Cedar Falls, Iowa, United States of America
mark.hecimovich@uni.edu
Phone: 1.319.273.6477
Abstract
Purpose: The purpose of this study was to measure concussion knowledge and awareness of youth Australian Rules Football players and parents. Secondary aims were examining if player’s maturity in age, history of concussion and years played and parents who have undergone first aid and concussion training would increase knowledge.
Methods: 1,441 parents and 284 youth ARF players completed a 23-item concussion knowledge survey consisting of three areas: concussion symptoms, management, and return-to-play criteria.
Results: There was significant difference in knowledge of concussion management and return-to play criteria between players and parents (p= less than 0.01). Players age, years played and history of concussion did not increase knowledge, however, parents with concussion training had significantly higher scores than those without (p= less than 0.01). Some return-to-play criteria and signs and symptom not thought to be associated with concussion such as disturbed sleeping and difficulty studying were difficult for both groups to associate as related to concussion.
Conclusions: Future concussion education opportunities for player and parents need to focus on return-to-play criteria and uncommon signs and symptoms such as sleep disturbances and problems studying.
Applications in sport: The findings reflect certain areas that need to be incorporated into educational opportunities for players and parents, especially those who have limited access to qualified health care professionals such as ATC’s. Although there is minimal evidence supporting concussion educational opportunities, awareness and knowledge of concussion is the greatest positive influence for symptom reporting among young athletes. However, the ideal delivery mode and educational content for interventions appropriate to each group has yet to be identified so steps such as defining the target group, measuring their level of awareness and knowledge, and monitoring of effectiveness. Overall, the goal should be to provide at least the basic information regarding concussion but as the results of this study demonstrate ensure lesser known aspects such as return-to-play criteria and signs and symptoms such as sleep disturbances and difficulty studying or concentrating are incorporated.
KEYWORDS: Concussion, awareness, youth, parent, Australian Rules Football
INTRODUCTION
As a subset of mild traumatic brain injuries (32) sport-related concussions have become an increasingly serious concern (9, 11, 30). As more information has emerged about the cause, course, and sequelae of concussion, the importance of greater awareness and knowledge for the recognition and management of concussion has improved (39).
Awareness of sport-related concussion is an es¬sential step in increasing the number of athletes or parents who report on concussion and proper clinical assessment and management (44). This awareness is important, in particular, for youth-level Australian Rules Football (ARF) where medical care at games and training may be limited to individuals with only first aid training or those with a weekend sports trainers certificate; certified athletic trainers (ATC) do not exist in Australia. However, this is also important in the United States as only 70% of public secondary schools have access to ATCs at sports games and practices and approximately two-thirds of all public secondary schools do not have a full-time athletic trainer (36). Additionally, there is no established data on ATC coverage available at youth-level American football. In this circumstance, aside from the coach, it is the players and parent who need to aware of possible signs and symptoms of concussion. Therefore, increased player and parent awareness is an important step toward progress in this area (33). Children are particularly susceptible to these injuries with 65% of all sport-related head injuries presenting to United States of America (USA) emergency departments being aged 5–18 years (5). In Australia, the impact of concussion on the child and on the health sector is not well described despite 63% of school-aged children participating in at least one organized sport outside school hours (3).
Although there are a number of sporting organizations that focus on improving care for possible concussion through their websites and freely provided materials (37), there appears to be a problem. This problem is with the transfer of information from the sporting organization to the individual clubs, coaches, parents and players, and the implementation of the recommendations. In the US, state laws mandate compliance with concussion education and return to play rules (37). Similar laws do not exist in Australia or in many other countries. Before considering legislative changes, the community, sporting clubs, and sporting organizations need to accept the problem and address the deficits in awareness and knowledge of sports related concussion (16).
In Australia, at the elite, professional level, both the Australian Football League (AFL) and the National Rugby League (NRL) recommend immediate removal from play, first aid management and assessment by medical personnel for athletes with suspected concussion (32, 1, 17). However, at the non-elite, non-professional level in Australian Football, the standard for junior or youth leagues is the requirement to have a person with current first aid qualifications available at all games (16). Unfortunately, this standard is a basic first aid course which may not allow sufficient training on concussion awareness. Therefore, it is vital to establish levels of concussion awareness for players, parents as well as coaches who participate in sports such as ARF in order to implement educational programs to increase awareness (40, 35).
The importance of greater awareness of concussion for parents was reported by King et al. (20) that showed 83 % of parents believed they could recognize a concussion in their teenager and 19 % would not have their teenager see a medical practitioner if there was a suspected concussion. However, the level of belief may fall short on actual levels of awareness and, therefore, baseline levels need to be established in order to measure the effectiveness of concussion awareness education. Gourley et al. (14) measured concussion awareness by youth players and parents with the results demonstrating only 3 of the 5 questions assessing recognition of proper concussion management were correctly answered by more than 70% by both groups. Additionally, less than 70% of youth athletes and parents correctly identified that an athlete should not return to play after a hit to the head. These results suggest that youth athletes and parents are moderately aware of the signs and symptoms of concussion and have little knowledge in proper concussion management. As a result of these findings there is a need to educate youth athletes and parents about seeking immediate medical care following a suspected concussion and the proper return-to-play criteria.
The findings reported by Gourley et al. (14) and King et al. (20) highlight the need for a greater awareness of concussion across players and parents. This awareness is important because in the absence of adequate medical coverage and inadequate coaching staff knowledge, awareness may ultimately fall on the parent and player. In undertaking this study, the broad aim was to measure the level of knowledge of concussion awareness in youth players and parents associated with ARF. This was undertaken to establish baseline knowledge levels that can be used in future studies to measure the effectiveness of educational opportunities. Secondary aims of this study were:
(1) To determine if a player’s maturity in age, and years played, would improve knowledge of concussion symptoms and if those who have sustained a concussion previously would have a greater understanding of concussion symptoms. This was determined to be beneficial as mature players may be able to assist in the education of younger players, who may be more prone to relate to the more experienced player; and
(2) To determine whether parents who have undergone first aid and concussion training, respectively, are able to recognize concussion symptoms at higher levels than those without. These items are components which can form future club/organization educational opportunities and easily implemented and therefore warrant inclusion and analysis.
METHODS
Youth ARF players and parents of players were the target population with this study having full support of the West Australia Football Commission (WAFC) and South West Regional Football Development Council. The WAFC invited current players and parents of current players to participate in the study. Institutional Review Board approval (2015/017) was obtained prior to conducting the study.
The study was a cross-sectional descriptive survey. Numerous concussion awareness and knowledge surveys were reviewed with the aim to select one that would require minor amendments and be appropriate for youth ARF players and parents of youth ARF players. For this study, youth was defined as age 19 and under. A concussion awareness survey to assess general knowledge of sport-related concussion for youth athletes and parents of youth athletes was selected (14). The survey was previously used in a similar study (14) conducted in the US with slight modifications from a 2007 study (42) and reported to have acceptable reliability (α = 0.83).
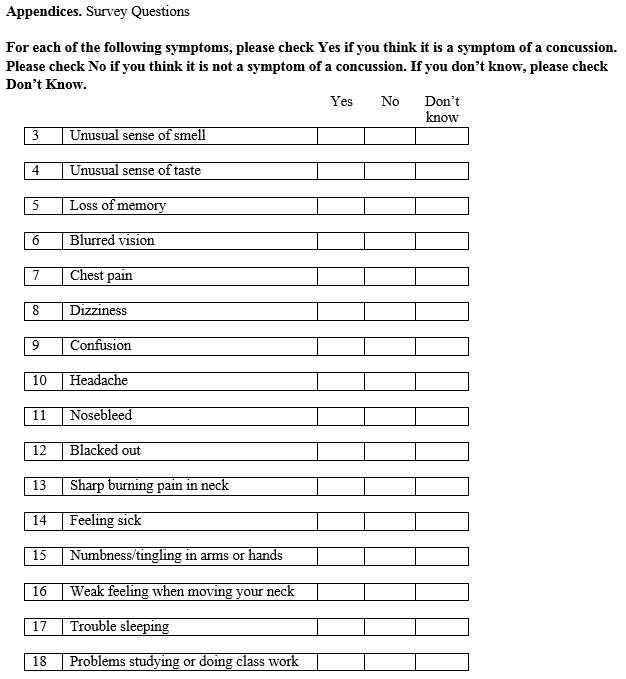
The survey consisted of demographic questions, and questions on three areas which have been reported to be important aspects of concussion awareness, 1) recognition of signs and symptoms, 2) concussion management, and 3) return-to-play criteria (42, 18, 27). Please refer to Appendix for survey items.
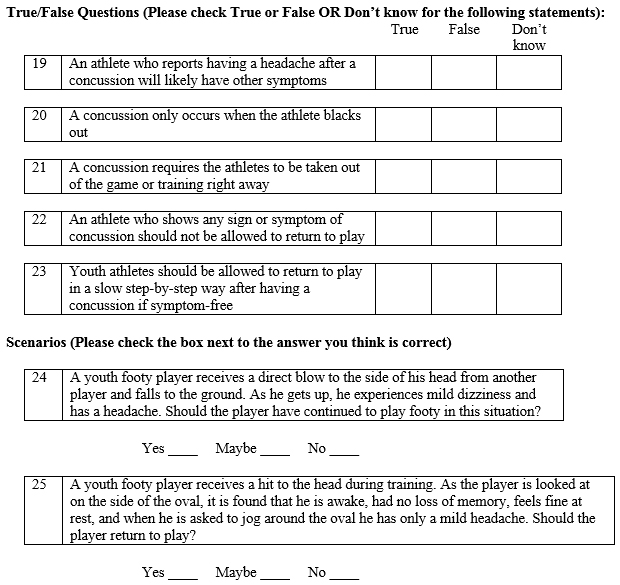
Sixteen items formed the Recognition of Signs and Symptoms (S&S) section and are the most commonly reported signs and symptoms of concussion (27, 28). Five items, in True-False (T/F) format, centered on a combination of concussion management and return-to-play and reported as important criteria on previous studies (22, 15, 31, 7, 21, 2). Response categories for these two sections were ‘Yes’, ‘No’, and ‘Don’t Know’. For scoring analysis, two categories were utilized, correct and incorrect with the ‘Don’t Know’ responses collapsed into the incorrect category. Collapsing ‘Don’t Know’ into incorrect responses typically will merge strong and weak effects, costing analytical precision. However, this was determined appropriate as the previous use of the survey utilized this method for analysis and feedback from experts in the field of sport-related concussion concluded that not knowing a reported sign or symptom of a concussion represented a high gravity of concern due to impact head trauma on health.
Two scenario items (Sc1 and Sc2) which centered on return-to-play criteria provided a brief description of an event (i.e., direct blow to the head) and resulting signs and symptoms and asking the respondent to determine the playability of the player. There were three response categories, ‘Yes’, ‘No’, and ‘Maybe’ with scoring of two categories for analysis being either correct and incorrect. The ‘Maybe’ responses were collapsed into the incorrect category.
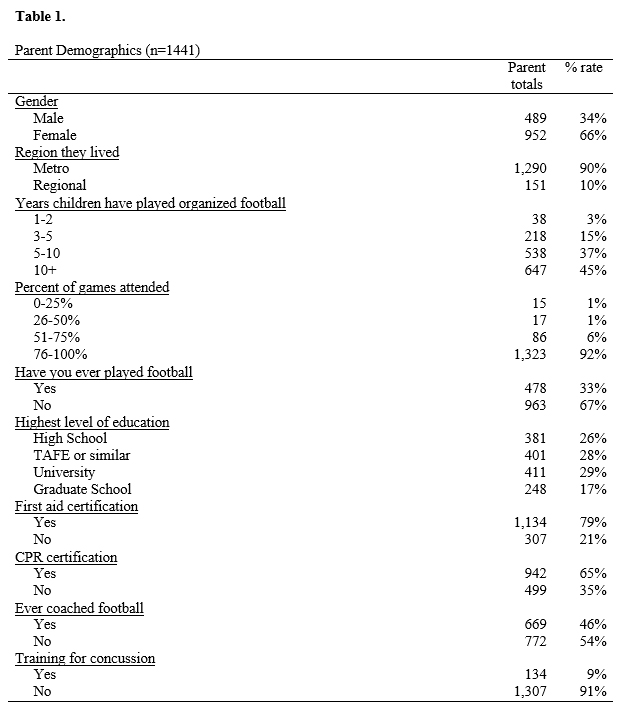
Each of the two scales (Parent and Player) had a demographic section. For the Parent scale (Ps), items included “how many years their children have played organized, coached, sports”, “what percentage of the games/competitions they attend”, and “level of education”. Also included were items aimed at determining their level of concussion awareness such as whether they had first aid training, and training specific for concussion. These items are components that can form future club/organization educational opportunities and easily be implemented and therefore warrant inclusion and analysis. The demographic section for the Player scale (PLs) included items on years participating in football, location (metropolitan, regional), and if they had ever had their ‘bell rung’ when playing football. No item pertained to previous concussion training was included as this was not the current policy at that time to have this available to players.
For this study, a review for content and face validity was undertaken by four experts in the field of sport-related concussion and two experts in the field of survey research. Slight amendments such as use of Australian terminology was incorporated and prior to administration a pilot study was performed using 7 youth ARF players (M=14.5 years old) and 6 parents of current ARF youth football players to assess clarity and provide feedback; no additional changes were suggested.
The 23-item survey was linked into the WAFC web site and made available to registered active youth football players and parents of current registered youth football players. The exclusion criteria were incomplete surveys and participants could only access the link once. Players and parents were invited by the WAFC to participate and informed consent were included at the beginning of the survey. The survey was made available from March through July 2015 with approximate number of players being 4100 and approximate number of parents being 6600. The numbers are approximate as final overall participant totals had not been established at that time and were in fluctuation due to dropout. Although the overall response rate is low compared to the number of players and parents, the large number of completed surveys is sufficient to have high confidence in the precision of the results presented below.
Statistical analysis was performed with IBM SPSS V.23. Frequency distributions were analyzed for the demographic data, scores on the Recognition of Signs and Symptoms section (S&S), True-False section (T/F), and each of the two scenario sections (Sc1 and Sc2). Given the non-symmetrical nature between groups, Mann-Whitney U tests were utilized to determine differences across the scores of the three sections.
Factorial analysis of variance was performed to compare scores on the S&S, T/F sections and each of the two scenario sections on players with a history of concussion, their age and how many years participating in sport. Analysis of variance were performed to compare parent S&S, T/F sections and each of the two scenario scores and first aid and concussion training, respectively. As there was an unequal sample size, Brown-Forsythe was utilized in the analysis. It was hypothesized that player’s maturity in age, and years played, would improve knowledge of concussion symptoms and those who have sustained a concussion previously would have a greater understanding of concussion symptoms and return-to-play scenarios. For parents, it was hypothesized that those who have undergone first aid and concussion training, respectively, are able to recognize concussion signs and symptoms at higher levels than those without.
RESULTS
Demographics
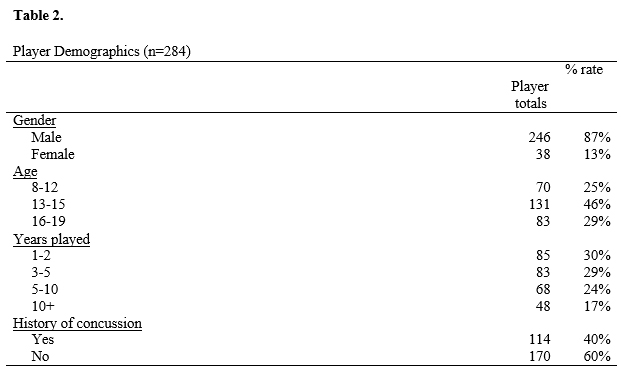
There were 1,441 parents and 284 players who responded to the survey. For players, 246 were male and 38 were female, and 40% reported a history of concussion. For parents, 79% had first aid training while 9% reported specialized training for concussion. Overall demographic data are presented in Tables 1 and 2.
Comparisons between players and parents
Scores of the S&S section, with similar distributions, showed no significant difference (p=.186) between players (M=10.38) and parents (M=10.28). However, for the T/F section, which had similar distributions, results between players (M=3.95) and parents (M=3.75) indicated a significant difference (p= less than.001). This also seen for the first scenario question (Sc1), which had similar distributions, that showed scores for players (M=.85) being significantly (p= less than .001) lower than parents (M=.94). For Sc2, distributions were not similar and scores for players (mean rank = 692.77, M=0.45) were significantly lower (p= less than.001) than parents (mean rank = 898.55, M=0.69).
Effect of player variables
The results showed no significant main effects and three-way interaction effect for age, years played, and history of concussion for the S&S (p=.917) and T/F scores (p=.884). The Sc1 score showed a significant interaction effect for age and years played (p = .019) but no significant three-way interaction effect for age, years played, and history of concussion (p = .333). The results for the Sc2 score showed no significant main effect and three-way interaction effect for age, years played, and history of concussion and Sc2 (p = .441).
Effect of parent variables
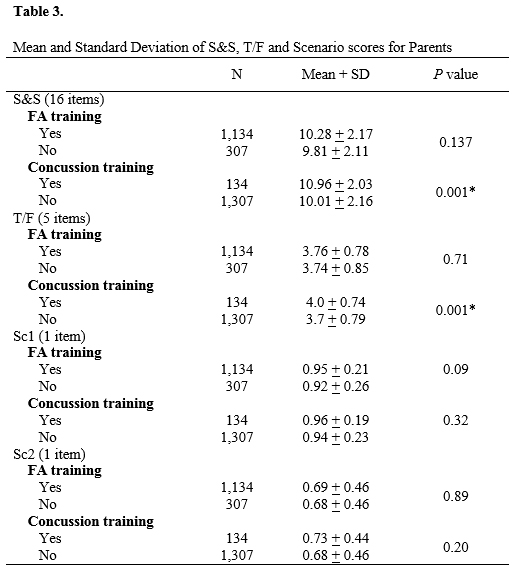
First aid (p=.001) and concussion training (p=.001) had a significant effect on the S&S results. For the T/F sections scores, first aid training (p=.712) did not result in a significant difference, whereas concussion training did (p=.001). However, neither first aid (Sc1: p=.060; Sc2: p=.891) nor concussion training (Sc1: p=.319; Sc2: p=.204) had an effect on the scenarios (Table 3).
Overall player and parent responses
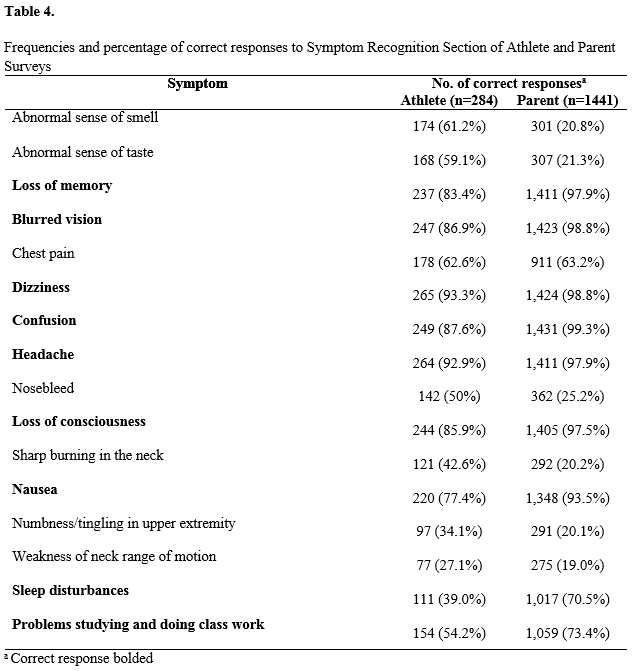
Responses on the S&S items are listed in Table 4. Key areas to note are players and parents recognizing loss of memory (Pl 83%, P 98%), blurred vision (Pl 87%, P 99%), dizziness (Pl 93%, P 99%), confusion (Pl 88%, P 99%), headache (Pl 93%, P 98%), and loss of consciousness (Pl 86%, P 98%) as possible concussion signs and symptoms at high level. Two areas which get little mention and not often associated with concussion, disturbed sleeping and difficulty studying, were correctly identified by only 39% and 54% of players, and 70% and 73% of parents, respectively.
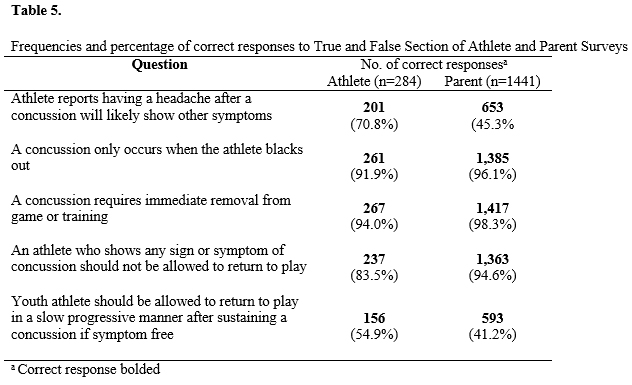
Knowledge on concussion management with return-to-play (T/F) (Table 5) showed two areas which proved difficult. The first, whether an athlete who reports having a headache after a concussion will likely show other symptoms, was incorrectly identified by almost 30% of players and 54% of parents. The second, whether a youth athlete should be allowed to return to play in a slow progressive manner after sustaining a concussion if symptom free, had less than 55% of athletes and 41% of parents recognizing this as being proper concussion management.
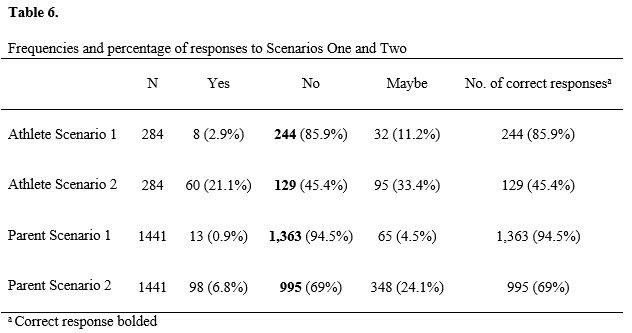
Results for the scenario return-to-play (Sc1 and Sc2) (Table 6) showed players and parents correctly identified the first scenario at a higher level (Pl 86%, P 94%) than the second (Pl 55%, P 31%), which asked when a player only has mild headache after receiving a hit to the head, should they be able to return to play.
DISCUSSION
Comparisons between players and parents
The current study revealed significant difference between player and parent awareness of concussion management (T/F items) and return-to play criteria (Sc1 and Sc2). Conversely, there were no significant difference in symptom recognition (S&S).
For concussion management with return-to-play criteria, formatted in the T/F items, players (M=3.95) had greater awareness than parents (M=3.75). The reason for this could be that although instruction on concussion for Australian sports trainers is rudimentary in comparison to ATCs, and coaches possess a fair base of knowledge on concussion (43) the higher scores reported in players may be the result of them having more direct contact with the sports trainers and coaches. The findings do differ than Gourley’s et al. (14) US survey which reported no differences. In their study, 3 of the 5 concussion management questions were correctly answered by more than 70% of youth athletes and parents whereas in the current study 4 questions were correctly answered by more than 70% of players, and parents; notably 3 correctly answered by more than 90% of parents. Interestingly, although the T/F items did contain elements of return-to-play, parents scored significantly higher in the scenario-based return-to-play items in comparison to players. The reasons for this may be item interpretation or players having previously experienced the scenarios with no detrimental effects which may have impacted their responses.
Effect of player and parent variables
Our hypothesis that a players age, participation experience in years and a previous history of concussion would increase their knowledge and awareness was not the case except for the first scenario. The results could be due to lower concussion rates in ARF in comparison to other similar codes such as American football (12). Lower number of players experiencing concussion, in other words actual scenarios of concussion, are relatively small (12) and the 40% of players in this study indicating a previous history of concussion may not have truly sustained one and therefore lack actual experience.
For parents, those who reported having had some form of concussion training had significantly higher scores than those without such training. Although no specific details were obtained on the training, the results support the importance of these educational opportunities which is further supported by established empirical evidence (13). However, results from the current study also suggest that even parents with some concussion training have difficulty recognizing concussion symptoms and therefore the importance of more in-depth educational programs aim at the novice level.
Responses on combination of concussion management with return-to-play
Two items in this section (T/F) need to be incorporated in concussion education programs. The responses for the first item, should a youth athlete be allowed to return to play in a slow progressive manner after sustaining a concussion if symptom free, showed a low number of players (55%) and parent (43%) not knowing this was true. This low level of awareness could be due to return-to-play management getting limited attention in educational material available to players and parents. This area is typically a medical or coaching decision but in the absence of sufficient medical staff available at games and practices, educational programs need to incorporate this component. However, there is a misconception even among the majority of coaches and a significant proportion of sports trainers that players can return to normal training once they are symptom free (43). Although remaining symptom free is a crucial component of the AFL and NRL return-to-play guidelines, the guidelines also stipulate that players should return-to-play gradually, using a stepwise approach (43). Therefore, even if parents and players are receiving information, it may be from ill-informed medical professionals, such as sports trainers, and coaches.
The second item, whether an athlete who reports having a headache after a concussion will likely show other symptoms, was correctly identified by only 70% of players and only 45% of parents. Causes of headache may be difficult to interpret as players may experience one for numerous reasons (i.e., inadequate hydration level) and therefore confusion exists about its association with other signs and symptoms. Although research (23) has found that 75% of collegiate athletes who reported a headache following a concussion also reported a minimum of 1 other concussion symptom, such as dizziness and confusion.
Responses on return-to-play
In the scenario section (Sc1 and Sc2), which pertained to return-to play criteria, parents had significantly higher scores than players overall but both scored very high in scenario 1 (a youth footy player receives a direct blow to the side of his head from another player and falls to the ground. As he gets up, he experiences mild dizziness and has a headache. Should the player have continued to play footy in this situation?). For scenario 2, which asks whether a player should return to play after receiving a hit to the head but is awake, has no loss of memory, feels fine at rest, and when asked to jog around the oval has only a mild headache, only 45% of players and 69% of parents correctly answered that the player should not return to play. This reflects a lack of understanding on the seriousness of headache, even if mild. Although, as will be discussed in the next section, there was a high awareness of headache being an important indicator of concussion (S&S section) the concern is the level of headache as it pertains to return-to-play criteria; in this case, mild. This information is vital as concussed athletes who return to play while still symptomatic have an increased risk of recurrent injury and associated complications (41, 32). However, despite the largest sporting codes adopting best practice concussion management guidelines, only 7% of parents or children associated with Australian sport are aware of any pre-injury concussion instructions or return-to-play guidelines from their sporting organization, suggesting current implementation of the guidelines is inadequate (16).
Responses on signs and symptoms
Players and parents had high recognition of commonly reported signs and symptoms such as loss of memory, blurred vision, dizziness, confusion, headache and loss of consciousness, which is consistent with research on youth athletes and parent of youth athletes (14, 8). Two areas which were not recognized highly by players and parents were sleep disturbances and problems studying; the latter being recognized less with players in comparison to a similar US study (37) on high school athletes. This is an important issue as awareness of potential educational deficit is critical for athletes to recognize and to ensure proper recovery (34) as cognitive demands could increase symptom severity as well as length of recovery time (26). For sleep disturbances, recent investigations have identified the presence of certain physical signs and clinical symptoms during the acute phase of a concussion as potential identifiers of a protracted recovery (24, 25) and therefore may not be well understood in the sporting community.
There are several limitations with this study. It is important to acknowledge that surveys bias respondents based on interest in the survey topic; respondents who may have been more interested, better trained, or less trained (and looking for training) may been more apt to participate. A low response rates which may have impacted the results and the omission of on item for prior first aide and concussion training was based on this not being a required standard, but some clubs may be providing their own. The surveys were completed in an unsupervised environment so partici¬pants were not able to ask for help in understanding the survey questions. The differing results for scenario-based items (T/F and scenarios) seem to indicate that there was some difficulty understanding there complexi¬ty and it is possible that some of the young¬er players may not have fully understood some of the questions, and that this may have added some error to our estimates. Future studies may benefit from distributing the sur¬veys to youth athletes and their parents at orientation meetings at the beginning of the season so the investigator can supervise completion. Lastly, it needs to be stressed that players may experience any or all of approximately 21 disparate symptoms and conceptualizing concussion in a ‘one size fits all’ approach to does not address the highly individualized nature of this injury and can result in ineffective management and educational strategies (6).
CONCLUSIONS
The primary aim was to establish baseline levels of knowledge and awareness of youth players and parents associated with ARF on concussion with the view that these measurements can be used in future studies to examine the effectiveness of educational opportunities. From this study it is clear that these opportunities need to focus on areas such as return-to-play criteria and greater emphasis on uncommon signs and symptoms such as sleep disturbances and problems studying. As individual player’s maturity and years played did not improve levels of knowledge and parents who had previous concussion training still had difficulty recognizing certain signs and symptoms, the call for on-going yearly concussion training is also highly recommended.
APPLICATION TO SPORT
The participants this study did well overall but the findings reflect certain areas that need to be incorporated into educational opportunities for youth players and parents, especially those involved in impact sports such as a ARF, American football and rugby. This is particularly true where there is limited access to qualified health care professionals trained in concussion management such as ATC’s.
Areas which need to be incorporated into concussion training include uncommon signs and symptoms such as sleeping difficulty and problems studying. Both players and parents need to be aware of these two important issues. Sleep disorders are common after a person sustains a concussion and prompt identification and treatment are an important part of the recovery process. Sleep is critical to the brain’s healing and recovery processes. During this recovery time, the brain is not functioning at full capacity, and this can impact how a player tolerates life developments and their education. It is vital, after a concussion, that parents, teachers, and medical personnel collaborate to not only ensure an uneventful recovery but also pace learning at a speed appropriate for the brain’s recovery. This is important as pushing too hard too early will frustrate the individual and possibly cause long term effects to learning ability.
Another area which needs to be incorporated into educational opportunities is formulating various scenarios of game or practice play in combination of signs and symptoms. The combination of the two may produce a better way for players and parents to think about signs and symptoms as opposed to the memorizing a list.
Although there is minimal evidence supporting concussion educational opportunities, awareness and knowledge of concussion is the greatest positive influence for symptom reporting among young athletes (19). Often players do not know how a concussion could affect them and sometimes do not think it warrants reporting, but concussion education helps young athletes identify what qualifies as a concussion (19). Important to note is research (38, 4, 29) has shown that player concussion-reporting behaviors are negatively influenced depending on fear of losing playing time, game-versus-practice situation, not having a medical professional available, and letting others down. This shows the importance of having appropriate personnel, trained in the management and care of sport related concussions, available to adolescent athletes. However, in the absence of trained medical personnel, or when concussive injuries occur outside of athletics, adequate player and parent understanding of its importance is required.
The ideal delivery mode and educational content for interventions appropriate to each group (i.e., youth player, parents, coaches, administrators) has yet to be identified so these need to be carefully considered. However, prior to implementing concussion education opportunities, the target group (i.e., youth player and parent) needs to be defined. Once done, the group’s current level of awareness and knowledge has to be measured; as this study did as its primary aim. Once these two components are complete, the appropriate method of delivery needs to be determined. For example, population-specific videos which are easy to administer and provides a message that crosses over gender and sport, using multiple learning styles including visual, verbal, and somatosensory to enhance knowledge of concussive injury. Other methods of delivery include: face-to-face with medical personnel or former athletes and printed material. However, as learning strategies are changing, for example the use of social media (Facebook and Twitter), these approaches need to be scrutinized to ensure that the proper information is communicated. This can be accomplished through the use of routine monitoring of effectiveness such as yearly surveys. Finally, it is important that the educational opportunities be implemented on a yearly basis to reflect the changing attitudes of players as they get older and the seriousness of sport increases.
Overall, the goal should be to provide at least the basic information regarding concussion (what is a concussion; how do I know I [my child/my athlete] have/has a concussion; symptom recognition; whom to report to; and the consequences of the injury) but as the results of this study demonstrate ensure lesser known aspects such as return-to-play criteria and signs and symptoms such as sleep disturbances and difficulty studying or concentrating are discussed.
ACKNOWLEDGEMENTS
We thank the West Australia Football Commission (WAFC) and South West Regional Football Development Council for their support of this project. There was no funding for this project.
REFERENCES
1. AFL Research Board, AFL Medical Officer’s Association. Guidelines for the management of concussion in Australian football for general practitioners. Available from: http://www.aflcommunityclub.com.au/index.php?id=66[accessed 09.10.15].
2. Aubry M, Cantu R, Dvorak J, Graf-Baumann T, Johnston K, Kelly J, et al. (2002). Summary and agreement state¬ment of the First International Conference on Concussion in Sport, Vienna 2001. Recommendations for the improvement of safety and health of athletes who may suffer concussive injuries. Br J Sports Med., 36, 6-10.
3. Australian Bureau of Statistics. 4901.0 – children’s participation in cultural and leisure activities, Australia, Organised Sports, 2009. Available from:http://www.abs.gov.au/ausstats/abs@.nsf/Products/4901.0∼Apr+2009∼Main+Features∼Organised+sport?OpenDocument [accessed 09.03.15].
4. Bramley H, Patrick K, Lehman E, & Silvis M. (2012). High school soccer players with concussion education are more likely to notify their coach of a suspected concussion. Clin Pediatr., 51(4), 332–336.
5. Centers for Disease Control and Prevention. (2011). Nonfatal traumatic brain injuries related to sports and recreation activities among persons aged ≤ 19 years – United States, 2001–2009. MMWR, 60(39), 1337–42.
6. Collins M, Kontos A.P., Reynolds E, Murawski C.D., & Fu F.H. (2014). A comprehensive, target approach to the clinical care of athletes following sport-related concussion. Knee Surg Sports Traumatol Arthrosc,, 22, 235–246. DOI 10.1007/s00167-013-2791-6.
7. Collins M, Stump J, & Lovell M. (2004). New developments in the manage¬ment of sports concussion. Curr Opin Orthop., 15, 100-107.
8. Cournoyer J, & Tripp B.L. (2014). Concussion Knowledge in High School Football Players. J Athl Train., 49, 654–658. doi: 10.4085/1062-6050-49.3.34.
9. Covassin T, Elbin R III, & Sarmiento K. (2012). Educating coaches about concussion in sports: evaluation of the CDC’s ‘‘Heads Up Concussion in Youth Sports’’ initiative. J School Health, 82(5), 233–8.
10. Cusimano M. (2009). Canadian minor hockey participants’ knowledge about concussion. Can J Neurol Sci., 36, 315-320.
11. De Beaumont L, Brisson B, Lassonde M, et al. (2007). Long-term electrophysiological changes in athletes with a history of multiple concussions. Brain Inj.,21(6), 631–44.
12. Fortington L.V., Twomey D.M., & Finch CF. (2015). Concussion in community Australian football – epidemiological monitoring of the causes and immediate impact on play. Injury Epidemiology, 2(20): doi:10.1186/s40621-015-0052-5.
13. Glang A.E., Koester M.C., Chesnutt J.C., Gioia G.A., McAvoy K, Marshall S, & Gau J.M. (2015). The Effectiveness of a Web-Based Resource in Improving Postconcussion Management in High Schools. J Adol Health., 56, 91-97.
14. Gourley M.M., Valovich-McLeod T.C., & Bay R.C. (2010). Awareness and Recognition of Concussion by Youth Athletes and Their Parents. Athlet Train Sport Health Care., 2(5), 208-218.
15. Guskiewicz K, Bruce S, Cantu R, Ferrara M, Kelly J, McCrea M, et al. (2004). National Athletic Trainers’ As¬sociation position statement: Management of sport-related con¬cussion. J Athl Train., 39:280-297.
16. Haran H, Bressan S, Oakley E, Davis G, Anderson V, & Babl F. (2015). On-field management and return-to-play in sports-related concussion in children: Are children managed appropriately? J Sci Med Sport. http://dx.doi.org/10.1016/j.jsams.2015.02.009.
17. International Rugby Board. IRB concussion guidelines. Available from:http://www.irbplayerwelfare.com/?documentid=3 [accessed 05.04.14].10.
18. Kaut K, DePompei R, Kerr J, & Congeni J. (2003). Reports of head injury and symptom knowledge among college athletes: Implications for assessment and educational intervention. Clin J Sport Med., 13:213-221.
19. Kay M.C., Welch C.E., & Valovich-McLeod T.C. (2015). Positive and Negative Factors That Influence Concussion Reporting Among Secondary-School Athletes. J Sport Rehabil., 24(2), 210-3. doi: 10.1123/jsr.20130132.
20. King D, Brughelli M, Hume P, & Gissane C. Assessment, Management and Knowledge of Sport-Related Concussion: Systematic Review. Sports Med., 44, 449–471. DOI 10.1007/s40279-013-0134-x.
21. Kissick J, & Johnston K. (2005). Return to play after concussion: Principles and practice. Clin J Sport Med., 15, 426-431.
22. LaBotz M, Martin M, Kimura I, Hetzler R, & Nichols A. (2005). A comparison of preparticipation evaluation history form and a symptom-based concussion survey in the identification of previous head injury in collegiate athletes. Clin J Sport Med., 5, 73-78.
23. LaBotz M, Martin M, Kimura I, Hetzler R, & Nichols A. (2005). A comparison of a preparticipation evaluation history form and a symptom-based concussion survey in the identification of previous head injury in collegiate athletes. Clin J Sport Med., 15, 73-78.
24. Lau B.C, Collins M.W, & Lovell M.R. (2012). Cutoff scores in neurocognitive testing and symptom clusters that predict protracted recovery from concussions in high school athletes. Neurosurgery, 70(2), 371-379.
25. Lau B.C., Kontos A.P., Collins M.W., Mucha A, & Lovell M.R. (2011). Which on-field signs/symptoms predict protracted recovery from sport-related concussion among high school football players? Am J Sports Med., 39(11), 2311-2318.
26. Majerske C.W., Mihalik J.P., Ren D, Collins M.W., Reddy C.C., Lovell M.R, et al. (2008). Concussion in sports: postconcussive activity levels, symptoms, and neurocognitive performance. J Athl Train., 43:265-274.
27. Makdissi M, Darby D, Maruff P, Ugoni A, Brukner P, & McCrory P. (2010). Natural history of concussion in sport: markers of severity and implications for management. Am J Sports Med., 38, 464–71.
28. Meehan W.P., d’Hemecourt P, Comstock R.D. (2010). High school concussions in the 2008–2009 academic year: mechanism, symptoms, and management. Am J Sports Med., 38, 2405–9.
29. McCrea M, Hammeke T, Olsen G, Leo P, & Guskiewicz K. (2004). Unreported concussion in high school football players. Clin J Sport Med., 14, 13–17. PubMed doi:10.1097/00042752-200401000-00003.
30. McCrory P. (2011). Sports concussion and the risk of chronic neurological impairment. Clin J Sports Med., 21(1), 6–12.
31. McCrory P, Johnston K, Meeuwisse W, Aubry M, Cantu R, Dvorak J, et al. (2005). Summary and agree¬ment statement of the 2nd International Conference on Concus¬sion in Sport, Prague 2004. Clin J Sport Med., 15, 48-55.
32. McCrory P, Meeuwisse W, Aubry M, et al. (2012). Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med, 47(5), 250–8.
33. McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, et al. (2009). Consensus statement on concussion in sport—the 3rd International Conference on Concussion in Sports held in Zurich, November 2008. Br J Sports Med.,43(suppl 1), i76-i90.
34. Miyashita T.L., Diakogeorgiou E, Hellstrom B, Kuchwara N, Tafoya E, & Young L. (2014). High School Athletes’ Perceptions of Concussion. Ortho J Sport Med., 2(1), 2325967114554549. DOI: 10.1177/2325967114554549.
35. O’Donoghue E, Onate J, Van Lunen B, & Peterson CL. (2009). Assessment of high school coaches’ knowledge of sport-related concussion. Athl Train Sports Health Care.,1(3), 120–32.
36. Pryor R, Casa D, Vandermark L, Stearns R, Attanasio S.M., & Fontaine GJ. (2015). Athletic training services in public secondary schools: a benchmark study. J Athlet Train. , 50(2), 156–162. doi: 10.4085/1062-6050-50.2.03
37. RCW 28A.600.190 Youth sports – concussion and head injury guidelines – injured athlete restrictions – short title, Washington State Legislature. Available from: http://apps.leg.wa.gov/rcw/default.aspx?cite=28A.600.190 [accessed 09.04.15].
38. Register-Mihalik J.K., Linnan L, Marshall S, Valovich McLeod T, Mueller F, & Guskiewicz K. (2013). Using theory to understand high school aged athletes’ intentions to report sport-related concussion: Implications for concussion education initiatives. Brain Inj., 27, 878–886. PubMed doi:10.3109/02699052.2013.775508.
39. Rosenbaum A.M., & Arnett P.A. (2010). The development of a survey to examine knowledge about and attitudes toward concussion in high-school students. Journal of Clinical and Experimental Neuropsychology, 32(1), 44-55.
40. Sawyer R, Hamdallah M, White D, Pruzan M, Mitchko J, & Huitric M. (2010). High school coaches’ assessments, intentions to use, and use of a concussion prevention toolkit: Centers for Disease Control and Prevention’s Heads Up: Concussion in high school sports. Health Promot Pract.,11, 34-43.
41. Shrey, D.W., Griesbach G.S., & Giza C.C. (2011). The pathophysiology of concussions in youth. Phys Med Rehabil Clin N Am., 22(4), 577–602.
42. Valovich-McLeod T.C., Schwartz C, & Bay R.C. (2007). Sport-related concus¬sion misunderstandings among youth coaches. Clin J Sport Med.,17, 140-142.
43. White P.E., Newton J.D., Makdissi M, Sullivan S.J., Davis G, McCrory P, et al. (2014). Knowledge about sports-related concussion: is the message getting through to coaches and trainers? Br J Sports Med., 48, 119–124.
44. Yang J, Phillips G, Xiang H, Allareddy V, Heiden E, & Peek-Asa C. (2008). Hos-pitalizations for sport-related concussions in US children aged 5 to 18 years during 2000-2004. Br J Sports Med., 42, 664-669.