Submitted by Brandon Spradley, Sutthanuch Wiriyanpinit and Amber Magner
ABSTRACT
Purpose: Athletic trainers and sport medicine professionals have the responsibility of diagnosing and managing concussion in athletes. The King-Devick (K-D) Test provides athletic trainers and sport medicine professionals with an easy-to-use concussion screening tool that requires only two minutes to administer and has relevance to contact sports such as football, soccer, boxing, and mixed martial arts. The purpose of this pilot study was to examine the reliability of baseline testing with the K-D Test in different environments.
Methods: A total of nine participants (6 males, 3 females, mean age: 39 ± 14.49 yrs) participated in the three day investigation. Subjects reported to the human performance laboratory on three separate days. Participants were given standard instructions for the K-D Test. Participants were required to complete the K-D test under a quiet environment (with minimal to no noise) and under two loud (noisy) environments; one with speakers and the other with headphones.
Results: Results indicated K-D scores for baseline (BL) and speakers (SP) rendered group means of (BL: 40.54 ± 14.95 s, SP: 40.54 ± 15.92 s), while scores for HP signified slightly lower group means of 39.54 ± 14.39 s. No variables showed any statistical difference in K-D scores (P > 0.05).
Conclusion: Most participants were able to improve their K-D scores from Trial 1 (T1) to Trial 2 (T2) on baseline testing, signifying a slight learning effect within the study group.
Application to Sport: Athletic trainers, healthcare professionals, and those administering the K-D Test should be consistent in assessing pre and post K-D scores, although significant changes might not occur when performing the K-D Test under different environments (with crowd noise). Athletes should be treated on an individual basis when using the K-D Test to assess pre and post test scores.
INTRODUCTION
Millions of sport-related concussions occur in the United States every year at the youth, interscholastic, collegiate, and professional sport levels. Although the concussion injury rate continues to increase annually, sport-related concussions often go undiagnosed [5]. Athletic trainers and sport medicine professionals have the responsibility of diagnosing and managing these injuries in athletes. Even though concussion management has improved over the past decade, there has still been difficulty in establishing a single “gold standard” test to accurately assess sport-related concussions [5]. Various concussion tests have been used to assess concussions in athletes: Immediate Post-Concussion and Cognitive Testing (ImPact) [20], the Military Acute Concussion Evaluation (MACE) [3], and Sport Concussion Assessment Tool (SCAT) [21], with sport concussion management recommendations advocating a multi-facet approach [5].
Recent research demonstrates the need for a rapid screening test to assess concussion in athletes [7]. The King-Devick (K-D) Test is based on the measurement of rapid number naming and captures impairments of eye movements, attention, language, and other areas that correlate with suboptimal brain function [13]. The K-D Test provides athletic trainers and sport medicine professionals with an easy-to-use concussion screening tool that requires only two minutes to administer [7, 8]. Recent investigations [7, 8] have demonstrated the K-D Test as an accurate and reliable method for identifying athletes with head trauma. The test is a strong candidate for rapid sideline screening and has particular relevance to contact sports such as football, soccer, hockey, boxing, and mixed martial arts [7, 8].
With the K-D Test being an effective screening tool and practical in both competitive and practice settings, testers should understand the reliability of this assessment in different environments and conditions. If in fact the K-D Test is a functional sideline screening tool, the test should be reliable in both loud and quiet environments. Many athletic trainers who have utilized the K-D Test have administered the test in environments with minimal to no noise. If an athlete has suffered a head injury in competition, the environment in which the athlete will undergo testing would most likely be loud (noisy); considering crowd noise and the many other elements in athletic competitions. While the K-D Test is a very accessible and usable concussion screening tool, it is imperative for athletic trainers to consider the different environments in which this test is administered upon. Since the validity of the K-D Test is highly based on pre and post test scores, athletic trainers or those administering this assessment should be cognizant of the effects different conditions could have on athletes’ K-D Test scores. Therefore, the purpose of this pilot study was to examine the reliability of baseline testing with the K-D Test in different environments.
METHODS
Participants
A total of nine participants (6 males, 3 females, mean age: 39 ± 14.49 yrs) participated in the three day investigation. The research study was approved by an Institutional Review Board for the use of human subjects, and all subjects signed an informed consent prior to the investigation. Subjects were required to abstain from consuming any alcoholic beverages 24 hours prior to testing. Convenient sampling was used to recruit subjects. All participants were employees and/or doctoral students at the United States Sports Academy.
The King-Devick (K-D) Test
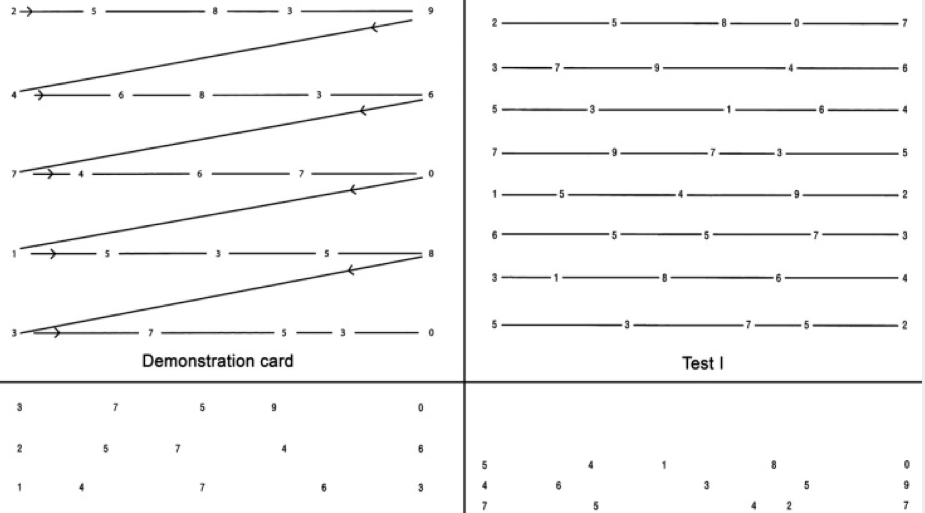
The K-D Test is based on the time to perform rapid number naming [16, 18]. The test involves a total of four test cards, one demonstration card and three test cards (Figure 1). Each test involves reading aloud a series of single digit numbers from left to right [7, 8]. Only the three test cards are scored and recorded. Each test card is structured and spaced differently to increase the difficulty of reading each test card. The individual administering the test should emphasize to the subject that each card should be read as quickly as possible without making any errors. The K-D Test requires saccadic eye movement; therefore subjects are not allowed to use their hands or fingers to complete the test. All testing should be recorded with a standardized stopwatch. The tester should start the stopwatch when the subject reads the first number and stop the watch when the last number has been read. The tester should monitor and record any errors made from each test card. Baseline scores are determined by the fastest time in which the subject completed the test without any errors.
Figure 1: King-Devick Test demonstration and testing cards
Study Design
Subjects reported to the human performance laboratory on three separate days. Participants were given standard instructions for the K-D Test. The K-D Test was completed a total of three times; each time in a different environment. Testing arrangements (seating, testing placement, lighting, etc) were consistent throughout the duration of the study. On the first day of testing, subjects were required to complete the K-D Test under a quiet environment (minimal to no noise). Baseline scores for each participant were derived from this protocol and used to compare K-D scores with the other variables. The next day of testing, subjects were required to complete the K-D Test under a loud (noisy) environment. Two types of testing variables were implemented to replicate an environment that would be similar to that of a sports competition. Audio crowd noise was downloaded to a computer to mimic the noise heard in most sport competitions. Subjects were required to complete this testing protocol twice: once while listening to the crowd noise with headphones and once while listening with speaker phones. Volume was set to mid-level on both the computer and the speakers to ensure a reasonable noise level for the participants. Randomization was used to choose which protocol each participant underwent on the second day of testing. Subjects completed the last testing treatment on the third day of testing. All testing was completed between the hours of 11:00 a.m. to 2:00 p.m. for the purpose of keeping the time consistent throughout the testing. The characteristics of each subject while performing the K-D test under each treatment were also recorded throughout the duration of the testing. Subjects were instructed to complete each treatment twice for a total of two trials for each variable assessed in the study.
Data Analysis
All tests were analyzed using a one-way analysis of variance (ANOVA) and dependent t-tests. The One-way ANOVA and the dependent t-test were used to compare the means of each variable to examine whether any statistical difference was observed. A p-value less than 0.05 was considered significant for this investigation. Statistical analysis were performed using the computer program SPSS (PASW Statistics 18.0.0, IBM Corporation, Armonk, NY, USA).
RESULTS
K-D group results are shown in Table 1. Results indicated K-D scores for baseline (BL) and (speakers) SP rendered group means of (BL: 40.54 ± 14.95 s, SP: 40.54 ± 15.92 s), while scores for headphones (HP) signified slightly lower group means of 39.54 ± 14.39 s. No variables showed any statistical difference in K-D scores (P > 0.05) (Figure 2). Individual participant responses for (BL to SP) demonstrates an even spread of participants who either increased or decreased from BL scores to SP scores, whereas all the participants except one decreased K-D scores from BL to HP. Individual responses for each variable can be observed in Figure 3.
Table 1
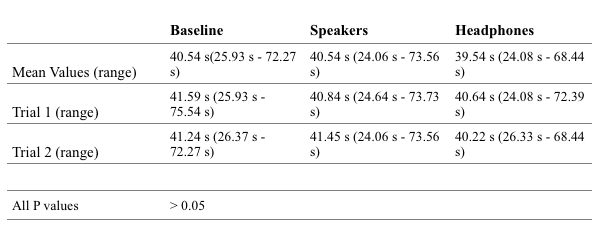
Figure 2: Group means of K-D scores for each variable. BL = Baseline, SP = Speakers, HP = Headphones. Significance set a P > 0.05. No significant differences were observed.
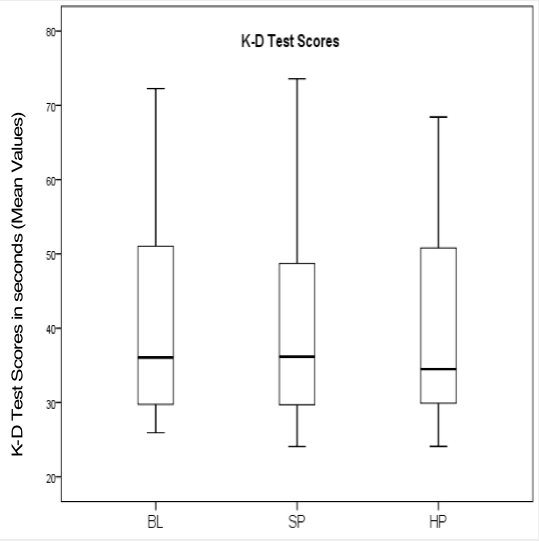
Figure 3: Individual participant responses for all variables: assessing changes from baseline testing to speakers and baseline testing to headphones. ∆ = Delta Values (Treatment – Baseline). Dashed lines represent K-D score group means. SP = Speakers, HP = Headphones.
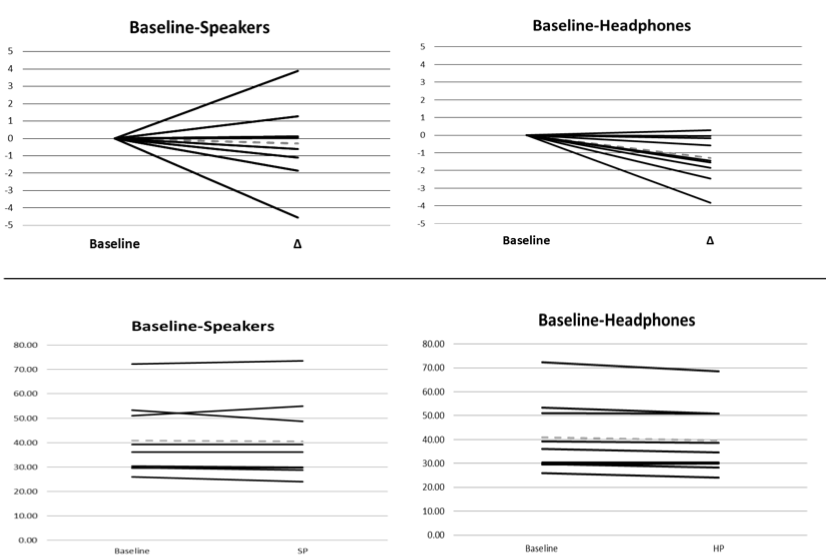
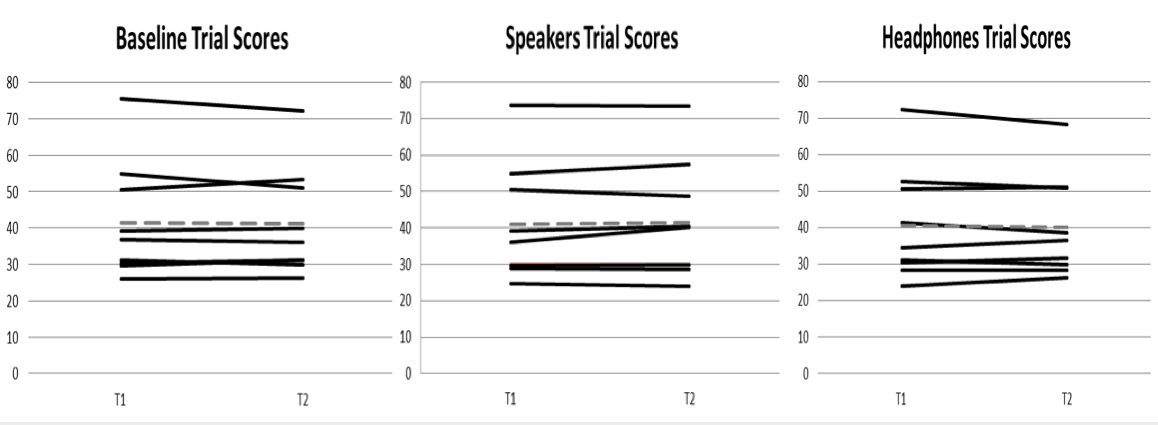
Results also indicated slight decreases (improvements) in K-D scores from Trial 1 (T1) to Trial 2 (T2) for BL and HP (BL: T1 mean: 41.59 ± 16.04 s, T2 mean: 41.24 ± 14.93 s; HP: T1 mean: 40.64 ± 15.46 s, T2 mean 40.22 ± 13.96 s). Participants K-D scores increased (worsened) when undergoing the testing protocol with SP (SP: T1 mean: 40.83 ± 16.01 s, T2 mean: 41.45 ± 16.08 s). No significant differences were observed from T1 to T2 with any of the variables assessed in the study (p > 0.05). Individual responses for T1 to T2 for each variable can be observed in Figure 4.
Figure 4: Individual participant responses for all variables: assessing changes from Trial 1 (T1) to Trial 2 (T2). Dashed lines represent K-D score group means.
DISCUSSION
This pilot study was the first to examine participants K-D baseline scores in different environments. The results suggest that the K-D Test is a reliable tool that can be used for baseline testing in quiet and loud environments.
The K-D Test has an advantage over other concussion assessments being that it is portable and easily adaptable for sideline administration [8]. This screening tool is based on the measurement of the speed of rapid number naming [16, 18] with a purpose of assessing concussions in athletes who may have incurred head trauma in athletic competitions or practices. The K-D Test captures eye movements, attention, language, and other areas that correlate with suboptimal brain function in which the brainstem, cerebellum, and cerebral cortex are all involved in these processes [7, 16, 18]. Saccadic and other types of eye movements are frequently abnormal following concussion, and eye movement function may serve as a predictor of post-concussion syndrome [13].
Many concussion assessment tools are still in the research phase, although when fully developed should be available for widespread clinical use [5]. The K-D Test can be placed into this category with recent investigations establishing its effectiveness in identifying athletes with head trauma. In 2011, Galetta et al. [7] investigated the effectiveness of the screening tool for assessing concussions in a cohort of boxers and mixed martial arts fighters. Results showed a significant increase (worsening) in K-D scores for participants who incurred head trauma during competition (59.1 ± 7.4 vs. 41.0 ± 6.7 s). In addition, participants who lost consciousness had even higher post-fight test scores (65.5 ± 2.9 vs. 52.7 ± 2.9 s). This significant increase in K-D scores most likely stems from the brain not being able to function at a normal processing speed as it would if a concussion has not been experienced. Another study by Galetta et al. [8] used the K-D Test to determine the effect of concussion on K-D scores in a college cohort. Numerous (n = 219) male and female collegiate athletes were assessed in this study and competed in the following contact sports: varsity football, sprint football, soccer, and basketball. Similar to Galetta’s previous investigation, results indicated a significant worsening of athletes who experienced concussions compared to their baseline scores (post concussion: 46.9 s vs. baseline: 37.0 s, p = 0.009).
The K-D Test has shown slight learning effects in the past, which is also evident in the current pilot study. As a group, participants were able to decrease their K-D scores from T1 to T2 on both the BL and HP treatments (BL: T1 mean: 41.59 ± 16.04 s, T2 mean: 41.24 ± 14.93 s; HP: T1 mean: 40.64 ± 15.46 s, T2 mean 40.22 ± 13.96 s). It seems that participants are able to improve their K-D scores from becoming familiar with performing each test card. Interestingly, an increase in K-D group scores was observed in the SP treatment from T1 to T2 (SP: T1 mean: 40.83 ± 16.01 s, T2 mean: 41.45 ± 16.08 s). This observation, in compliance with the other results in the study suggest that learning effects and learning effect sizes are different in each participant and individual scores should be analyzed separately. Individual response for treatments can be seen in figure 4.
In the past, sport medicine professionals have relied on computerized neurocognitive testing to determine subtle cognitive changes in post-concussion athletes [11, 17]. As a recommendation for concussion management, Guskiewicz et al. [11] stated “although normative data exist for neurocognitive testing without a baseline, baseline testing is strongly recommended so athletes can serve as their own controls.” This advice applies to the K-D Test being that this particular screening tool, when observed from an individual scoring standpoint, has the potential to vary under various conditions and environments. Athletic trainers should be cognizant of the effects of different environments and must make the decision on which environment and under what conditions the K-D Test should be administered upon.
Results in the current pilot study showed no significant effects in K-D scores with a change in environments (increase in noise level). Although the environments in this study were not as practical as actual sport-like competition environments, this could give an indication of the specifics of what needs to be done in future studies assessing the K-D Test. K-D baseline testing that occurs in actual competition or practice settings could provide for more reliable scores; being that post testing will occur in similar environments. Galetta et al. [8] mentioned in their study that a refinement of study design features, including baseline testing on sidelines, testing in the setting of post-game fatigue, and testing of athletes without concussions during competitions or practices should be considered for future studies with the K-D Test.
Concussion is highly related to a constellation of signs and symptoms and requires a high index of suspicion on the part of athletic trainers [5]. Furthermore, some signs and symptoms of concussion may not be present immediately, but may evolve over several hours to days after a concussive episode [5]. Being that the K-D Test captures many aspects of brain functions, including subcortical pathways that extend beyond eye movements, this test may help coaches and trainers with game decisions regarding the removal of an athlete who may have been concussed [7]. Thus, just as other research studies [7, 8] have mentioned, the K-D Test is a strong candidate for a rapid sideline screening tool for assessing concussion in sport-related events.
CONCLUSION
The overall findings of this pilot study indicate that no significant differences were observed when participants performed the K-D Test in different environments. Results also support that most participants were able to improve their K-D scores from T1 to T2 on baseline testing, signifying a slight learning effect within the study group. This suggests that participants who underwent prior testing with the K-D Test were more consistent and efficient in baseline values when comparing both trials (T1 and T2).
APPLICATION TO SPORT
Athletic trainers, healthcare professionals, and those administering the K-D Test should be consistent in assessing pre and post K-D scores, although significant changes might not occur when performing the K-D Test under different environments (with crowd noise). In addition, those performing the K-D Test should be given familiarization testing to provide each participant with more consistent K-D scores. Athletes should be treated on an individual basis when using the K-D Test to assess pre and post test scores (Figure 3 and 4). Therefore, it is imperative that athletic trainers recognize the effect that different environments/conditions may have on each individual. All in all, athletic trainers should remember the following important elements when assessing athletes with this assessment: proper data collection procedures, individual responses in athletes, accurate timing, and identification of testing errors.
ACKNOWLEDGMENTS
None
REFERENCES
- Broglio, S. P., Ferrara, M. S., Macciocchi, S. N., Baumgartner, T. A., & Elliott, R. (2007). Test-retest reliability of computerized concussion assessment programs. Journal of athletic training, 42(4), 509-514.
- Broglio, S. P., Macciocchi, S. N., & Ferrara, M. S. (2007). Neurocognitive performance of concussed athletes when symptom free. Journal of athletic training, 42(4), 504-508.
- Coldren, R. L., Kelly, M. P., Parish, R. V., Dretsch, M., & Russell, M. L. (2010). Evaluation of the Military Acute Concussion Evaluation for use in combat operations more than 12 hours after injury. Military medicine, 175(7), 477-481.
- Covassin, T., Stearne, D., & Elbin, R. (2008). Concussion history and postconcussion neurocognitive performance and symptoms in collegiate athletes. Journal of athletic training, 43(2), 119-124.
- Eckner, J. T., & Kutcher, J. S. (2010). Concussion symptom scales and sideline assessment tools: a critical literature update. Current sports medicine reports, 9(1), 8-15.
- Eden, G. F., Stein, J. F., Wood, M. H., & Wood, F. B. (1995). Verbal and Visual Problems in Reading Disability. Journal of Learning Disabilities, 28(5), 272-290.
- Galetta, K. M., Barrett, J., Allen, M., Madda, F., Delicata, D., Tennant, A. T., . . . Balcer, L. J. (2011). The King-Devick test as a determinant of head trauma and concussion in boxers and MMA fighters. Neurology, 76(17), 1456-1462.
- Galetta, K. M., Brandes, L. E., Maki, K., Dziemianowicz, M. S., Laudano, E., Allen, M., Balcer, L. J. (2011). The King-Devick test and sports-related concussion: study of a rapid visual screening tool in a collegiate cohort. Journal of the neurological sciences, 309(1-2), 34-39.
- Guskiewicz, K. M., & Broglio, S. P. (2011). Sport-related concussion: on-field and sideline assessment. Physical medicine and rehabilitation clinics of North America, 22(4), 603-617.
- Guskiewicz, K. M., Bruce, S. L., Cantu, R. C., Ferrara, M. S., Kelly, J. P., McCrea, M., . . . McLeod, T. C. (2004). Recommendations on management of sport-related concussion: summary of the National Athletic Trainers’ Association position statement. Neurosurgery, 55(4), 891-895.
- Guskiewicz, K. M., Bruce, S. L., Cantu, R. C., Ferrara, M. S., Kelly, J. P., McCrea, M., . . . Valovich McLeod, T. C. (2004). National Athletic Trainers’ Association Position Statement: Management of Sport-Related Concussion. Journal of athletic training, 39(3), 280-297.
- Heitger, M. H., Jones, R. D., & Anderson, T. J. (2008). A new approach to predicting postconcussion syndrome after mild traumatic brain injury based upon eye movement function. IEEE Engineering in Medicine and Biology Society. Conference, 2008, 3570-3573.
- Heitger, M. H., Jones, R. D., Macleod, A. D., Snell, D. L., Frampton, C. M., & Anderson, T. J. (2009). Impaired eye movements in post-concussion syndrome indicate suboptimal brain function beyond the influence of depression, malingering or intellectual ability. Brain : a journal of neurology, 132(10), 2850-2870.
- Ira, K. (2004). Educating the educators: increasing grade-school teachers’ ability to detect vision problems. Optometry – Journal of the American Optometric Association, 75(7), 445-451.
- Langlois, J. A., Rutland-Brown, W., & Wald, M. M. (2006). The epidemiology and impact of traumatic brain injury: a brief overview. The Journal of head trauma rehabilitation, 21(5), 375-378.
- Maruta, J., Suh, M., Niogi, S. N., Mukherjee, P., & Ghajar, J. (2010). Visual tracking synchronization as a metric for concussion screening. The Journal of head trauma rehabilitation, 25(4), 293-305.
- Notebaert, A. J., & Guskiewicz, K. M. (2005). Current trends in athletic training practice for concussion assessment and management. Journal of athletic training, 40(4), 320-325.
- Oride, M. K., Marutani, J. K., Rouse, M. W., & DeLand, P. N. (1986). Reliability study of the Pierce and King-Devick saccade tests. American journal of optometry and physiological optics, 63(6), 419-424.
- Reddy, C. C., & Collins, M. W. (2009). Sports concussion: management and predictors of outcome. [Review]. Current sports medicine reports, 8(1), 10-15.
- Schatz, P. (2010). Long-term test-retest reliability of baseline cognitive assessments using ImPACT. The American journal of sports medicine, 38(1), 47-53.
- Shehata, N., Wiley, J. P., Richea, S., Benson, B. W., Duits, L., & Meeuwisse, W. H. (2009). Sport concussion assessment tool: baseline values for varsity collision sport athletes. British journal of sports medicine, 43(10), 730-734.
