Abstract
Sports should prevent athletes from having eating disorders not develop eating disorders. There is evidence that female athletes are at a risk of developing
disordered eating. The purpose of this study was to find how prevalent eating disorders are in female athletes and examine factors that may have a relationship
with eating disorders.
A questionnaire containing two instruments was distributed to volunteer female athletes in a Midwestern university. The EAT 26 was used to measure the prevalence
of eating disorders. The ATHLETE questionnaire was used to inquire some factors that may have a relationship with eating disorders among athletes. Results showed
14.3% of the respondents scored a 20 and above on the EAT 26 and thus considered at risk of having an eating disorder. The ATHLETE questionnaire showed that
there were some significant negative correlations between the EAT 26 score and participant’s feelings about their body, feelings about sports, feelings
about performance, and feelings about eating. The negative correlations meant that the more the participants scored high on their feelings about their body,
sports, performance, and eating, the less likely they scored low on the EAT 26 indicating they did not have a risk of an eating disorder.
This study implies that when athletes feel good about their body, sport, performance and their eating, the less likely they will have an eating disorder. This study
makes an important contribution in understanding female athletes and eating disorders as well as factors that may have a relationship to eating disorders
in female athletes.
Introduction
An eating disorder is a psychological disorder that many women can acquire, ncluding collegiate athletes. Participation in sports activity can be a healthy
and enjoyable experience that can enhance self-worth and self-image in female athletes (12). Many people may believe that because athletes participate in
sports and maintain high levels of physical activity, they are not as self-conscience about their bodies. Contrary to this belief, (1) stated in their study that
athletes are at a greater risk for developing eating disorders than non-athletes. Why female athletes have eating disorders when they are so active is a question
of interest to many people. The purpose of this study is to find how prevalent eating disorders are in female athletes and examine factors that may have a
relationship with eating disorders.
Incorrect weight perceptions are more common in young women, with persistent overestimation of weight and attempts to lose weight even when unnecessary (7).
(5) stated that female athletes are a group particularly at risk for developing eating disorders or engaging in unhealthy behaviors to control their weight.
These athletes not only face the typical social pressures to be thin, but they also are immersed in a social context that focuses on their bodies.
Eating disorders are behavioral syndromes associated with considerable mobility that present onset of the highest mortality rates among mental illnesses. The
prevalence of eating disorders’ has increased since the 1990s in both female athletes and non-athletes. Female athletes go through a lot of pressures
and conflicts playing collegiate sports. Female athletes are a group particularly at risk for developing eating disorders or engaging in unhealthy behaviors to
control their weight (13).
The western cultural emphasis given to weight and body shape points towards a “beauty standard” centered on thinness disorders (11). For some
female college athletes, college concerns and pressures may contribute to eating disorders or disordered eating behaviors (6). The sports environment can heighten
body and weight related concerns because of factors such as pressure from coaches and social comparisons, body dissatisfaction, physique anxiety, and perfectionism
(6, 11). A lack of professional guidance can make an athlete vulnerable to the onset of disordered eating (10). It appears that negative moods such as anxiety,
perfectionism, and negative comments about body shape or weight from coaches are related to disorder eating in female athletes (1). (9) found that social
pressure on body shape was strongly correlated with body dissatisfaction. Female athletes’ body dissatisfaction has shown correlation with bulimia (6).
According to (7), perfectionism, for example in sports has been found to be a risk factor for bulimic symptoms.
However, prevalence of clinical and subclinical eating disorders has been found to be higher-among female athletes than non-athletes (5). Young women, particularly
those in aesthetic sports are vulnerable to body dissatisfaction, eating disorders, and disordered eating (10). Situational factors specifically involvement in
individual sports or team sports, may put athletes in situations where social physique anxiety and disordered eating is likely to be heightened to manage
weight and shape concerns (13, 8).
This is an important topic because although physical activity enhances self-esteem and promotes physical and emotional well-being, there is evidence that female
athletes are at a risk of developing disordered eating. It is important to investigate some of the reasons why female collegiate athletes feel the need to have disordered
eating. Results of the study can assist in developing and executing suitable eating-disorder prevention and intervention programs for female college athletes.
The purpose of the study was twofold. First, it was to assess how prevalent eating disorders were among female college athletes. Secondly, it was to explore
some factors that may have a relationship with eating disorders.
Methods
Participants
There were 56 participants in total, including 11 freshman, 21 sophomores, 13 juniors and 11 seniors. The following sports were included: soccer (23.2%),
softball (23.2%), track and field (41.1%), and swimming (12.5%). The age range was between 18 to 22 years, with over 98% being between 18 and 21 years. The
entire sample was Caucasian with an exception of one participant.
Instruments
A questionnaire was used to collect data, it included a demographic section on age, sex, height, weight and race of the participants. Two instruments were
included in the questionnaire, the first being the EAT 26 by (4), which measured prevalence of eating disorders among athletes. The EAT 26 has been used extensively
in research as a reliable measure of prevalence of eating disorders. The EAT-26 scale is comprised of these dimensions: dieting, bulimia and food preoccupation,
and oral control. Each item on the scale is rated on a scale of 0-6 as follows: never=0, rarely=0, sometimes=0, often=1, usually=2, and always=3, except for
item 25 which is reverse scored.
Second was the ATHLETE questionnaire, which was used to inquire some factors that may relate with eating disorders among athletes. The ATHLETE questionnaire
is a reliable and valid measure of factors that may relate to disordered eating in athletes (9). The ATHLETE questionnaire has the following factors that have
shown association with disordered eating: feelings about being an athlete, the athlete’s body and sports, feelings about performance, team support, feelings
about one’s body, and feelings about eating.
Both instruments showed acceptable reliability. The EAT 26 included 26 items and yielded a reliability value of .76. The six factors in the ATHLETE questionnaire
demonstrated the following reliability values: feelings about being an athlete included five items with a reliability of .71, athlete’s body and sports
included 12 items with a reliability of .87, feelings about performance included seven items with a reliability of .67, team support included four items with
a reliability of .73, feelings about one’s body included six items a reliability of .85, and feelings about eating included four items with a reliability of
.85.
Procedures
The researchers first obtained Human subjects approval from the IRB before conducting the study. The questionnaire was distributed to the participants, and it contained
the demographic section of the questionnaire, the EAT 26, and the ATHLETE questionnaire. The questionnaire was given to volunteer female athletes at a Midwestern university.
A volunteer female athlete served as the monitor and distributed the questionnaires. The study was conducted in the absence of the coach and the researchers so that
the participants would not feel any coercion to participate in the study. The consent information for the participants was included at the beginning of the
questionnaire. The consent information explained that participating in the study was totally voluntary and that by completing the questionnaire, the participant
was giving consent to participate in the study. The questionnaire was completed anonymously and since there were no signed informed consent it was not possible
to identify individuals who participated in the study nor those whose scores indicated they were at risk of an eating disorder. Due to the sensitive nature
of the study, all participants were provided with referral information to their school’s health center and the crises hotline center, in case they realized
they were at risk of acquiring an eating disorder.
Statistical analysis
The data was entered into SPSS program – PASW Statistics 18. Reliability test for the EAT 26 and the ATHLETE questionnaire was analyzed. Descriptive statistics
were analyzed for the EAT 26. Those who scored EAT 26=20 were considered at risk of having an eating disorder. ANOVAs were computed to compare the means
of EAT 26 by year in school, age, weight, and sport participation. Correlations were completed between the EAT 26 and the factors of the ATHLETE questionnaire.
Results
There were 56 total participants who responded to the questionnaire. Frequencies were completed for EAT 26. If the participant scored EAT 26=20, then they were
considered at risk of having an eating disorder. Results showed that 8 female athletes, (14.3%) scored a 20 and above and were thus considered at risk of
having an eating disorder. The EAT 26 mean was 7.9 and standard deviation was 7.6. Figure 1 shows details of how the participants responded to the EAT 26.
ANOVAs were used to compare the means of EAT 26 by classification year, age, weight, and sports participation. Only age showed a significant difference in
means for the EAT 26. Further, Cross tabs were completed between those who had EAT26=20 and age. Results showed all of the 8 participants who had EAT 26=20
were 19 years of age.
Descriptive statistics were conducted on how the female athletes performed on the ATHLETE questionnaire, which can be seen in Table 1. Pearson correlation
was conducted to see whether there was a relationship between EAT 26 and ATHLETE questionnaire factors.
These four factors in the ATHLETE questionnaire demonstrated significant Pearson correlation values with EAT 26: feelings about body and sports with a correlation
of -.53, feelings about performance with a correlation of -.51, feelings about your body with a correlation of -.50, and feelings about eating with a correlation
of -.31. These two factors in the ATHLETE questionnaire did not demonstrate significant Pearson correlation values with EAT 26: feelings about being an
athlete, and team support. Table 2 shows details about correlations between EAT 26 and the ATHLETE questionnaire factors.
Discussion
This study found 14.3 % of female athletes were considered at risk of having an eating disorder. This study also reported that everyone found to have an
eating disorder was 19 years old. The ATHLETE questionnaire showed that there were some significant negative correlations between the EAT 26 score and participant’s
feelings about their body, feelings about sports, feelings about performance, and feelings about eating. The negative correlations meant that the more the
participants scored high on their feelings about their body, sport, performance, and eating, the less they scored on the EAT 26, indicating they did not have
an eating disorder.
Two of the factors in the ATHLETE questionnaire dealt with body image; the athlete’s body and sports, and feelings about one’s body. Both factors
had a significant negative correlation with EAT 26 scores. This indicated that the female athletes’ who scored high on the athlete’s body and sports,
and feelings about one’s body were likely to score low on the EAT-26. Hence, indicating they were not likely to be at risk of an eating disorders.
This finding concurs with the study by (2), which contended that body image dissatisfaction is the strongest predictor of eating disorder symptoms.
A study done (6) stated that sport-related pressures such as weight limits, teammates’ eating-related behaviors, judging criteria, revealing uniforms,
and coach expectations have been suggested as potential risk factors for an athlete to develop an eating disorder. Our study found that team support and
feelings about being an athlete did not have a relationship with eating disorders. Another study done by (10) stated that families, peers, and coaches can have
a major effect on female athletes. Our study did not show that pressures from the participant’s families, peers, and coaches had any effect on the athlete
and eating disorders.
This study found that ‘feelings about performance’ in the ATHLETE had a significant negative correlation with the EAT 26 total. This indicated
that the more the athletes felt good about their performance in sports, the less likely they were at risk of an eating disorder. This finding concurs with
(1) study that stated that negative moods such as anxiety and perfectionism were related to disordered eating in female athletes.
In the current study, all participants who scored EAT 26=20, were 19 years old, and were either sophomores or juniors in school. There were no freshman
or seniors found to have a risk of an eating disorder. This indicates that the female athlete participants felt more pressure or problems with their eating
in the middle of their college years. This finding concurs with the study by (2), which stated that eating and dieting problems in college freshman women
was fairly stable across the first year of college. The current study suggests that the female athletes develop some eating disorder as they try to lose weight
in the sophomore year and stabilize by the fourth year. More research is needed on eating disorders of female athletes through the four college years.
Since the participants is this study was were nearly all Caucasian, this study may have found higher levels of disordered eating concerns than a more diversified
sample. Future similar studies can build on this study by having a larger proportion of other ethnicities. In addition, future similar studies can have a wider range
of sport, especially sports where the athletes’ uniforms for competition are more revealing such as swimming, dance, and gymnastics.
Conclusion
This study shows that eating disorders are prevalent among female athletes. Some factors that have a relationship with eating disorders include feelings
about their body, sports performance, and eating. This study also shows that feelings about being an athlete such as being competitive and team support did
not show much relationship with eating disorders.
This study makes an important contribution in understanding females and eating disorders, as well the factors that may have a relationship in causing eating
disorders in female athletes.
Application to Sport
Eating disorders are still an issue of concern among female athletes. This study reveals that the more female athletes felt good about their body, sports,
performance, and eating, the more likely they would not have an eating disorder. Feelings about an athlete like being competitive and team support did not show
much relationship with eating disorders. To keep away from disordered eating, female athletes ought to have positive inner feelings about themselves.
Sports participation among college females should be encouraged because this will improve their ‘feelings about their body’ and in turn make
them less at risk of getting an eating disorder. Participation in sports activity can be a healthy and enjoyable experience that can enhance self-worth and self-image
in female athletes (12). Since body image dissatisfaction is the strongest predictor of eating disorder symptoms (2), then body image holds the most promise as a
focus for prevention programs of eating disorder among college female athletes.
Disordered eating prevention efforts offered by college counseling centers for female athletes should focus on promoting students’ acceptance of their own
bodies. Such efforts will counteract the media influences that propagates the extremely ‘thin ideal’ that is unattainable by most normal female
athletes. A school-based sport centered program can be useful in deterring females from disordered eating (3). For those working with athletes, they should avoid
equating thinness to sport performance. They should be encouraged to become more knowledgeable and responsible regarding the critical role of healthy eating
and nutrition in female athletes. Such knowledge will equip them to play a significant role identifying, managing, and preventing eating disorders among female athletes
and increase prospects of a positive sport experience for female athletes. Female athletes ought to be encouraged to regard their health first before sports performance.
Consequently, the International Olympic Committee (IOC) emphasizes an athlete’s health rather than weight and body composition (12).
Acknowledgements
Many thanks to the anonymous volunteer female athletes who agreed to participate in this study.
References
1. Arthur-Cameselle, J., Quatromoni, P.(2011). Factors related to the onset
of eating disorders reported by female collegiate athletes. The Sport Psychologist,
25(1), 1-17.
2. Cooley, E., & Toray, T. (2001). Disordered Eating in College Freshman
Women: A Prospective Study. Journal of American College Health, 49(5), 229.
3. Elliot D, Goldberg L, Moe E, et al. (2004). Preventing substance use and
disordered eating: Initial outcomes of the ATHENA program. Arch Pediatric Adolescent
Medicine, 158:1043-1049.
4. Garner, D. M., Olmsted, M. P., Bohr, Y., & Garfinkel, P. E. (1982).
The Eating Attitudes Test: Psychometric features and clinical correlates. Psychological
Medicine, 12, 871–878.
5. Greenleaf, C., Petrie, T., Carter, J., Reel, J.(2009). Female collegiate
athletes: prevalence of eating disorders and disordered eating behaviors. Journal
of American College Health, 57(5) 485-495.
6. Greenleaf, C., Petrie, T., Reel, J., Carter, J. (2010). Psychosocial risk
factors of bulimic symptomatology among female athletes. Journal of Clinical
Sport Psychology, 4, 177-190.
7. Haase, A.(2011). Weight perception in female athletes: association with
disordered eating correlates and behavior. Eating Behaviors, 12,64-67. doi:
10.1016/j.eatbeth.2010.09.004.
8. Haase, A. (2009). Physique anxiety and disordered eating correlates in female
athletes: differences in team and individual sports. Journal of Clinical Sports
Psychology, 3, 218-231.
9. Hinton, P. S., & Kubas, K. L. (2005). Psychosocial Correlates of Disordered
Eating in Female Collegiate Athletes: Validation of the ATHLETE Questionnaire.
Journal of American College Health, 54(3), 149-156.
10. Kerr, G., Berman, E., Jane De Souza, M. J.(2006). Disordered eating in
women’s gymnastics: perspectives of athletes, coaches, parents, and judges.
Journal and Applied Sport Psychology, 18, 28-43. doi: 10.1080/10413200500471301.
11. Oliveria Coelho, G., Soares, E., & Ribeiro, B.(2010). Are female athletes
at increased risk for disordered eating and its complications. Appetite, 55,
379-387. doi:10.1016/j.appet.2010.08.003.
12. Sherman, R., & Thompson, R. A. (2006). Practical use of the International
Olympic Committee position stand on the female athlete triad; a case example.
International Journal of Eating Disorders, 39(3), 193-201. Doi:10..1002/eat.20232.
13. Sundgot-Borgen, J., & Torstviet, M.(2010). Aspects of disordered eating
continuum in elite high- intensity sports. Scandinavian Journal of Medicine
and Science in Sports, 20, 112-121. doi: 10.1111/j.1600-0838.2010.01190x.
14. Torstviet, M., Rosenvinge, J., & Sundgot-Borgan, J.(2008). Prevalence
of eating disorders and the predictive power of risk models in female elite
athletes: a controlled study. Scandinavian Journal of Medicine and Science in
Sports, 18, 108-118. doi: 10.1111/j.1600-0838.2001.00657x.
Figures and Tables
Fig 1- Eat 26 Performance
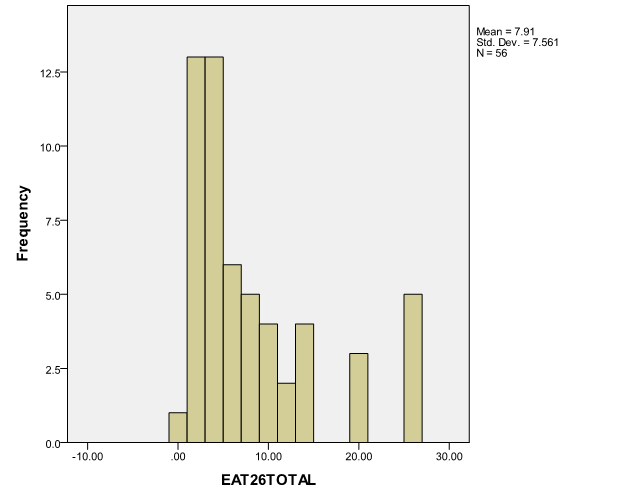
Legend: Figure 1 shows frequencies of the EAT 26 totals for the female athletes,N=56. If the participant scored EATS 26=20 then they were considered at risk
of having an eating disorder. Figure 1 shows that eight participants (14.3%) had EAT 26=20.
Table 2 – Descriptive Statistics of the ATHLETE Questionnaire
Legend: Table 2 shows the ATHLETE questionnaire which was used to inquire
some factors that may relate with eating disorders among athletes. The ATHLETE questionnaire
has six factors. Table 2 lists the six factors, sample questions on each factor,
as well as the descriptive statistics for the ATHLETE questionnaire.
| Factors of the ATHLETE questionnaire | Sample Question on the ATHLETE QUESTIONNIARE | No of Items | Total Possible | Mean | SD |
| Feelings about being an athlete | I cannot imagine what I will be like when I am no longer competing |
5
|
25
|
16.3
|
3.5
|
| The athlete’s body and sports | I would be more successful in my sport if my body looked better and I often wish I were leaner so I could perform better |
12
|
60
|
41.1
|
9.4
|
| Feelings about performance | No matter how successful I am, I never feel satisfied and my parents expect more of me athletically than I do for myself |
7
|
35
|
22.8
|
4.9
|
| Team support | It is hard to get close to my teammates because we are constantly competing against each other |
4
|
20
|
16.9
|
2.4
|
| Feelings about one’s body | My friends (non-athletes) make me feel I am too fat |
6
|
30
|
25.2
|
4.2
|
| Feeling about eating | I feel uncomfortable eating in front of my friends |
4
|
20
|
17.6
|
4.3
|
Table 3- Correlations between EAT 26 and the ATHLETE questionnaire
Legend: Table 3 shows the Pearson correlation values between EAT 26 and
the ATHLETE questionnaire factors. These four factors in the ATHLETE questionnaire
demonstrated significant Pearson correlation values with EAT 26; feelings about
body and sports; feelings about performance; feelings about your body; and feelings
about eating. These two factors in the ATHLETE questionnaire did not demonstrate
significant Pearson correlation values with EAT 26; feelings about being an
athlete, and team support.
| Factors of the ATHLETE questionnaire | Pearson Correlation With EAT 26 |
| Feelings about being an athlete | .139 |
| The athlete’s body and sports | -.530** |
| Feelings about performance | -.507** |
| Team support | .127 |
| Feelings about one’s body | -.502** |
| Feeling about eating | -.313* |
** .01 correlation is significant at the .01 level
*.05 correlation is significant at the .05 level
