Authors: Stephanie Choo1,3, Patrick Smith2, and James L. Cook1,3
1University of Missouri Department of Orthopaedic Surgery, Columbia, MO, USA
2Columbia Orthopaedic Group, Columbia, MO, USA
3Thompson Laboratory for Regenerative Orthopaedics, University of Missouri, Columbia, MO, USA
Corresponding Author:
James L. Cook, DVM, PhD, OTSC
William & Kathryn Allen Distinguished Chair in Orthopaedic Surgery
Director, Thompson Laboratory for Regenerative Orthopaedics & Mizzou BioJoint® Center
Chief, Orthopaedic Research Division
University of Missouri
Missouri Orthopaedic Institute (4028A)
1100 Virginia Ave
Columbia, MO 65212
(573) 884-4689
(573) 882-1760 fax
(573) 884-0603 lab
CookJL@health.missouri.edu
Stephanie Choo, MD is a second-year orthopaedic surgery resident in the Department of Orthopaedic Surgery and the Thompson Laboratory for Regenerative Orthopaedics at the University of Missouri. Her research interest is currently in the area of sports medicine with a focus on prevention and treatment of injuries in gymnastics.
Patrick A Smith, MD is an orthopaedic surgeon with the Columbia Orthopaedic Group and adjunct Professor of Orthopaedic Surgery for the University of Missouri. He specializes in arthroscopic surgery and sports medicine and has been involved in the care of athletes at Mizzou for more than 30 years.
James L. Cook, DVM, PhD, OTSC is the Allen Distinguished Chair, Professor, and Chief of the Division Orthopaedic Research at the University of Missouri, as well as Director of the Thompson Laboratory for Regenerative Orthopaedics. His areas of research encompass sports medicine, biologic joint restoration, tissue engineering, biomarkers, and osteoarthritis.
Use of Wrist Guards for Gymnasts – A Systematic Review
ABSTRACT
This systematic review was designed to provide the best current evidence regarding wrist guard use in gymnastics based on relevant biomechanical effects and injury prevention. Evidence supports the use of wrist guards as protective equipment in the prevention of gymnasts’ wrist pain and injury. However, potentially negative effects of wrist guards on proprioception and performance were also reported, and critical gaps in knowledge regarding guard design, most effective indications, and application to female gymnasts remain. Further biomechanical and clinical studies are needed to fill these gaps in knowledge toward making evidence-based recommendations regarding use of wrist guards in gymnastics.
Keywords: gymnastics, wrist pain, biomechanics, evidence-based recommendations
INTRODUCTION
Gymnastics is considered one of the highest-risk sports in the National Collegiate Athletic Association (NCAA) with respect to injuries (17). Among NCAA women’s sports, gymnastics reported the highest overall injury rate and practice injury rate (10.4 and 10.0 per 1,000 athletic exposures, respectively) (11). The high incidence of acute and chronic injuries in gymnasts has engendered a focus on repetitive loading biomechanics and protective mechanisms for injury prevention (4, 14, 17). Within this focus, the wrist is a key target based on frequency and severity of injuries. Studies have reported that 46% to 87.5% of gymnasts complain of wrist pain, likely attributable to repetitive, high-impact, axial compression loading and torsional stresses on the joint inherent to their activities (4, 16). Westermann and colleagues reported the wrist and hand to be the most injured body part in male gymnasts, the sixth-most injured area for female collegiate gymnasts, and the second-most frequently injured in the pediatric gymnastic population (17). Gabel categorized gymnastic wrist injuries into four types (acute, chronic, osseous, and soft tissue) with the most common involving distal radial physeal stress injuries, scaphoid impaction syndrome, dorsal impingement syndrome, triangular fibrocartilage complex (TFCC) tears, ulnar impaction syndrome, and lunotriquetral impingement (9).
Protective equipment and landing surfaces have been optimized to minimize ground reaction forces and reduce impact on gymnasts’ lower extremities (1, 12-13). Similarly, wrist guard use has been advocated by some authors based on biomechanical capabilities for restricting wrist hyperextension to prevent carpal abutment, dorsal impingement, and soft-tissue injuries using padding materials of various thicknesses in braces on the dorsum of the wrists (2-3, 5, 7). However, no clear evidence-based recommendations regarding use of wrist braces as protective equipment in the prevention of gymnasts’ wrist pain or injuries have been provided to the authors’ knowledge. Therefore, the purpose of this study was to systematically review available evidence regarding wrist guard use in gymnastics based on relevant biomechanical effects and injury prevention to determine critical gaps in knowledge towards optimizing wrist injury prevention for gymnasts.
METHODS
Three electronic databases—MEDLINE, PubMed, and EMBASE—were systematically searched using combinations of the keywords “gymnast,” “gymnastics,” “artistic gymnastics,” “wrist injury,” “wrist pain,” “wrist joint,” “wrist brace,” and “wrist guard” as terms, title words, and abstract words. Reference lists from identified articles were also reviewed for inclusion.
Studies in the English language and published between the years 1990 to 2020 were considered for inclusion. Studies were included when they provided data regarding wrist guard use in gymnastics, assessed biomechanical properties of wrist guards used in gymnastics, or evaluated injury prevention and efficacy of wrist guards in gymnastics. The title and abstract of each qualifying article were screened and full-text manuscripts were retrieved in cases of uncertainty for inclusion. The following data from included studies were then extracted: wrist support design, evaluation of injury prevention/efficacy of wrist support in gymnast, cadaveric, or biomechanical studies on wrist guards as it relates to the sport of gymnastics. PRISMA guidelines were used to determine final eligibility of papers included for systematic review. Two reviewers independently assessed risk of bias using the Cochrane Risk of Bias Tool.
RESULTS
The database search produced a total of 11 studies for review. A reference lists review produced an additional 8 relevant studies. On full review of these 16 articles, 3 met inclusion criteria for systematic review (Figure 1). One included study was a cadaveric biomechanical study, one was a single case report, and one was a prospective single-cohort case series. Qualitative synthesis of these 3 studies is provided below, including risk of bias assessment for each (Table 1).
Figure 1: Flowchart showing record review and study inclusion.
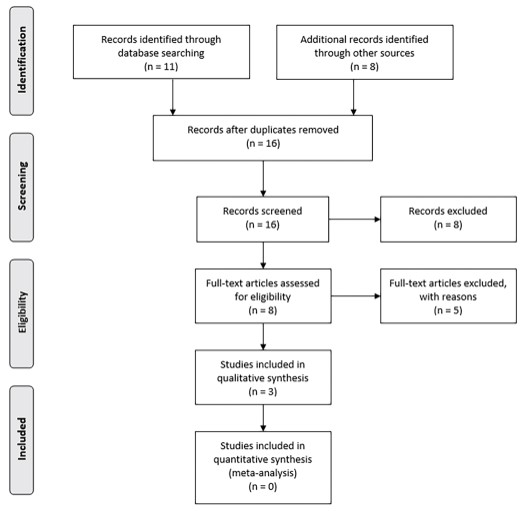
Table 1: Synthesis of Examined Studies
| Study Type | LOE | Risk for Bias | Clinical Relevance |
| Single Case Report | IV | Low risk | Athletic taping and wrist guard use may be a viable option for nonsurgical treatment of chronic wrist pain with Madelung deformity in gymnasts. |
| Prospective Single – Cohort Case Series | II | Intermediate risk Selection bias Attrition bias | Novel volar carpal force dissipation wrist brace significantly reduced wrist pain in male gymnasts (age 10-14, level 4-7) for floor, pommel, and parallel bars training. Novel brace negatively impacted proprioception and performance of older, higher-level male gymnasts. |
| Cadaveric Biomechanical Study | V | Low risk | The wrist brace with palmar pad significantly reduced wrist joint dorsiflexion angle and ulnocarpal joint peak pressure. Ulnocarpal joint peak pressures were 12% higher in females versus males. Prevention of pathologic wrist loading in gymnasts requires pressure attenuation intervention. |
Note. Information for the single case report is from the Journal of Athletic Training (2001), for the prospective single-cohort case series is from the Journal of Hand Therapy: Official Journal of the American Society of Hand Therapists (2020), and for the cadaveric biomechanical study is from The American Journal of Sports Medicine (2003)
Cadaveric Biomechanical Study
Grant-Ford et al. performed a cadaveric study to assess wrist guards (Ezy ProBrace, Gibson, Inc., Englewood, CO) designed for gymnasts (10). Twelve cadaveric upper extremities were tested in uniaxial tension-compression to simulate loading of the wrist during single-arm support of a 63 kg person. Ulnocarpal joint intraarticular peak pressure and wrist joint dorsiflexion angle data were collected for 3 test conditions: brace with palmar pad, brace without palmar pad, and non-braced. The brace, with or without palmar pad, significantly (p<0.05) reduced wrist joint dorsiflexion angle compared with the non-braced condition (non-braced angle, 87.5° +/- 4.1°, versus braced, 80.7° +/- 5.9° or 82.7° +/- 5.0°, with or without palmar pad, respectively). The decreased dorsiflexion angles were attributed to the brace design and material composition. The brace design used in this study was based on a lever arm 2.54 cm from the wrist and relatively stiff materials, including dorsal foam and rigid plate. The authors suggested that other brace designs and/or more pliable materials, such as athletic tape, would not have been associated with the same beneficial effects on wrist dorsiflexion. Furthermore, ulnocarpal joint intraarticular peak pressure was significantly lower with palmar pad than without palmar pad or in the non-braced control (110.5 +/- 13.5 mmHg versus 142.0 +/- 19.3 mmHg, p<0.05). Interestingly, ulnocarpal joint intraarticular peak pressures were 12% higher in female (148.1 +/- 26.6 mmHg) versus male cadaveric specimens (129.7 +/- 25.1 mmHg) (p<0.001). These data led the authors to conclude that prevention of pathologic wrist loading in gymnasts requires pressure attenuation intervention. Of note, the most common wrist guard brand reportedly used by competitive gymnasts (Tiger Paw, US Glove, Albuquerque, NM) is designed to reduce the dorsiflexion angle by dorsal support alone, in contrast to the biomechanically superior palmar-padded design evaluated in this study (18).
Single Case Report
One case report that supported the use of a wrist brace for conservative management of wrist pain in a collegiate gymnast met inclusion criteria (3). The report documented management of a female athlete presented at age 21 years for acute left wrist pain with a Madelung deformity. While Madelung deformity is typically corrected surgically in athletes with chronic pain and disability, Brooks et al. reported successful nonsurgical intervention using taping and wrist bracing in this case. The authors described a wrist taping method designed to prevent forceful end-range wrist extension using a palmar-fan, anchor strips to the forearm, and a continuous closure strip with a leather wrist brace over the tape. This combination of taping and bracing proved effective in preventing end-range left wrist extension while still allowing the athlete adequate mobility to successfully continue to compete at the collegiate level. The authors concluded that this combined wrist taping and bracing method can be considered for nonsurgical management of chronic wrist pain with Madelung deformity in competitive gymnasts.
Prospective Single-cohort Case Series
Trevithick et al. completed a prospective clinical trial to evaluate a newly designed wrist brace in a cohort of male gymnasts (15). The wrist brace evaluated differed from traditional designs that aim to restrict wrist hyperextension for reducing incidence of dorsal injuries, and instead focuses on mitigating volar compression forces acting on the wrist. This new design was based on biomechanical studies on wrist braces for snow sports that indicated volar-padded braces were effective in both load sharing and absorption of impact energy, dissipating the forces that contribute to ligament tears in low-energy impact falls onto an outstretched hand. To evaluate this design for gymnastics, the novel “volar carpal force dissipation wrist brace” was provided to 48 club and national level male gymnasts from 10 to 22 years of age who experienced wrist pain while performing gymnastics. The athletes completed a pain evaluation before the trial and immediately after using the novel wrist braces for 3 weeks of training. Pain was assessed with a visual analog scale of 0 to 10, before and after trial. The scale was defined as 0 = no pain, 1 to 5 = pain on activity that was relieved with rest, 6 to 9 = pain that remained present after activity ceased for up to 5 minutes after, and 10 = the pain prevented participation in the activity. The gymnasts reported three variables: 1) which apparatus was associated with wrist pain; 2) the level of pain experienced while training on the apparatus; and 3) where the wrist pain was located. The authors reported significant (p<0.05) decreases in pain in the mid dorsum (VAS score before 4.6 +/- 1.5, after 1.7 +/- 1.9; p= 0.05), mid volar (VAS score before 5.4 +/- 1.4, after 2.5 +/- 1.9; p= 0.03), and ulnar areas of the wrist (VAS score before 5.2 +/- 1.5, after 2.3+/- 2.1; p= 0.008) in association with 3 weeks of wrist brace use. However, radial-side pain was not significantly reduced with wrist brace use (VAS score before 5.0+/- 1.5, after 2.1 +/- 1.9; p= 0.07). The volar carpal force dissipation wrist brace significantly reduced wrist pain in 53.5% (p=0.002) of the athletes in level 4 to 7 (age 10 to 14 years) with training on the pommel, floor, and parallel bars. Importantly, higher-level gymnasts reported that the brace covering the palm negatively affected proprioception and performance technique by altering their speed and dexterity. In addition, female gymnasts were not included in this study cohort, limiting application of the results to the male gymnast population. Therefore, modifications to brace design and further studies are likely needed prior to making conclusions regarding routine use of this brace for gymnasts.
DISCUSSION
The systematic review of available evidence regarding use of wrist guards in gymnastics produced only 3 peer-reviewed articles that met inclusion criteria. The qualitative synthesis of these studies suggested that best current evidence supports protective biomechanical effects of wrist braces with palmar pads on dorsiflexion and ulnocarpal joint intraarticular peak pressure; potential for wrist taping and bracing as an effective non-surgical management technique for gymnasts’ chronic wrist pain, even with Madelung deformity; and volar carpal force dissipation wrist braces significantly mitigating wrist pain during training in male gymnasts.
Previous studies, including meta-analyses, have reported incidence and types of wrist injuries in gymnasts, but then only mention wrist brace use as a conservative management option without providing data regarding reduction of pain or prevention of injury (1-2, 4-5, 8-9). Gymnasts’ wrists are subjected to high-force repetitive loading across the radiocarpal and ulnocarpal joints and anecdotal recommendations for use of wrist bracing or taping in conjunction with alternating training activities to mitigate wrist pain and prevent injury (16). Despite these recommendations, up to 88% of gymnasts report experiencing wrist pain when training and competing, often lasting greater than a year (6)
Several studies in the peer-reviewed literature provide biomechanical assessments of wrist guards, but primarily focus on snowboarding and in-line skating with only 1 study found that specifically targeted the sport of gymnastics. The study reported biomechanical benefits of the wrist guard in significantly reducing dorsiflexion and ulnocarpal intraarticular joint loads, but only evaluated 1 type of wrist brace and only simulated forces generated during a pommel-horse skill, limiting its applicability (10). Still, these biomechanical studies provide important foundational data for understanding the functional kinematics and kinetics that must be addressed by effective wrist braces, serving as a catalyst for optimizing brace design to mitigate wrist pain and prevent injuries while maintaining comfort, function, and performance.
While only a single-case report, the documentation of successful use of a combination of taping and bracing for conservative management of chronic wrist pain with deformity to allow a female gymnast to continue to compete at the collegiate level is informative and encouraging (3). Madelung deformity of the wrist is typically surgically corrected in athletes with chronic pain and disability as was the case for the athlete described in this report. The use of taping and wrist bracing to successfully manage the patient nonsurgically provides further impetus for considering taping and bracing options for management of wrist pain and prevention of wrist injury in competitive gymnasts.
The prospective interventional study included in this systematic review suggests that use of a novel volar carpal force dissipation wrist guard can be an effective method for reducing pain in more than 50% of younger, lower-level male gymnasts after 3 weeks of use. Importantly, higher-level gymnasts reported negative effects on proprioception and performance, and female gymnasts were not included in the study. Interestingly, the wrist guard brand more commonly used currently by competitive gymnasts is a dorsal-support brace without palmar padding or volar support.
The primary limitation for this systematic review includes the extremely limited peer-reviewed literature available regarding wrist guard use in gymnastics that is focused on relevant biomechanical effects and injury prevention. In addition, the 3 studies meeting inclusion criteria were lower level of evidence studies, assessed different variations in wrist brace types with no consensus on most effective design, and were not broad in scope. As such, the data cannot be generalized in application, but rather are most useful for guiding modifications to brace design and strategies for further research.
CONCLUSION
Taken together, best current evidence supports the use of wrist braces as protective equipment in the prevention of gymnasts’ wrist pain and injury. However, potentially negative effects of wrist braces on proprioception and performance were also reported, and critical gaps in knowledge regarding brace design, most effective indications, and application to female gymnasts remain. As such, further biomechanical and clinical studies are needed to fill these gaps in knowledge toward making evidence-based recommendations regarding use of wrist guards in gymnastics.
APPLICATION IN SPORT
Based on the high prevalence of wrist pain and wrist injuries in gymnasts, it is imperative for athletes, coaches, trainers, parents, and physicians to recognize the extreme lack of evidence currently available for use of wrist guards, braces, and taping in this sport. The fact that this comprehensive, formal systematic review resulted in inclusion of only three peer-reviewed articles highlights the critical need for targeted research in this area of sports medicine. It is our hope that exposing this deficiency provides impetus and direction for completion of valid studies that shift the landscape in this area to one of evidence-based practice in the care of the millions of athletes who participate in gymnastics.
REFERENCES
- Arampatzis, Adamantios, Gaspar Morey-Klapsing, and Gert-Peter Brüggemann. 2005. “Orthotic Effect of a Stabilising Mechanism in the Surface of Gymnastic Mats on Foot Motion during Landings.” Journal of Electromyography and Kinesiology: Official Journal of the International Society of Electrophysiological Kinesiology 15(5): 507–15. https://doi.org/ 10.1016/j.jelekin.2004.12.002
- Benjamin, Holly J., Sean C. Engel, and Debra Chudzik. 2017. “Wrist Pain in Gymnasts: A Review of Common Overuse Wrist Pathology in the Gymnastics Athlete.” Current Sports Medicine Reports 16(5): 322–29. https://doi.org/10.1249/JSR.0000000000000398
- Brooks, Toby J. 2001. “Madelung Deformity in a Collegiate Gymnast: A Case Report.” Journal of Athletic Training 36(2): 170–73.
- Caine, Dennis J., and Larry Nassar. 2005. “Gymnastics Injuries.” Medicine and Sport Science 48: 18–58. https://doi.org/10.1159/000084282
- Chawla, Aditya, and Ethan R. Wiesler. 2015. “Nonspecific Wrist Pain in Gymnasts and Cheerleaders.” Clinics in Sports Medicine 34(1): 143–49. https://doi.org/10.1016/j.csm.2014.09.007
- DiFiori, John P., James C. Puffer, Bassil Aish, and Frederick Dorey. 2002a. “Wrist Pain, Distal Radial Physeal Injury, and Ulnar Variance in Young Gymnasts: Does a Relationship Exist?” The American Journal of Sports Medicine 30(6): 879–85. https://doi.org/10.1177/03635465020300062001
- DiFiori, John P., James C. Puffer, Bassil Aish, and Frederick Dorey. 2002b. “Wrist Pain in Young Gymnasts: Frequency and Effects upon Training over 1 Year.” Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine 12(6): 348–53. https://doi.org/10.1097/00042752-200211000-00005
- Dobyns, J. H., and G. T. Gabel. 1990. “Gymnast’s Wrist.” Hand Clinics 6(3): 493–505.
- Gabel, G. T. 1998. “Gymnastic Wrist Injuries.” Clinics in Sports Medicine 17(3): 611–21. https://doi.org/10.1016/s0278-5919(05)70104-6
- Grant-Ford, Marsha et al. 2003. “Effect of a Prophylactic Brace on Wrist and Ulnocarpal Joint Biomechanics in a Cadaveric Model.” The American Journal of Sports Medicine 31(5): 736–43. https://doi.org/10.1177/03635465030310051701
- Kerr, Zachary Y. et al. 2015. “College Sports-Related Injuries – United States, 2009-10 Through 2013-14 Academic Years.” MMWR. Morbidity and mortality weekly report 64(48): 1330–36. https://doi.org/10.15585/mmwr.mm6448a2
- Mills, Chris, Matthew T. G. Pain, and Maurice R. Yeadon. 2006. “Modeling a Viscoelastic Gymnastics Landing Mat during Impact.” Journal of Applied Biomechanics 22(2): 103–11. https://doi.org/10.1123/jab.22.2.103
- Mills, Chris, Maurice R. Yeadon, and Matthew T. G. Pain. 2010. “Modifying Landing Mat Material Properties May Decrease Peak Contact Forces but Increase Forefoot Forces in Gymnastics Landings.” Sports Biomechanics 9(3): 153–64. https://doi.org/10.1080/14763141.2010.524244
- Singh, Shubha, Gary A. Smith, Sarah K. Fields, and Lara B. McKenzie. 2008. “Gymnastics-Related Injuries to Children Treated in Emergency Departments in the United States, 1990-2005.” Pediatrics 121(4): e954-960. https://doi.org/10.1542/peds.2007-0767
- Trevithick, Beverly, Rebecca Mellifont, and Mark Sayers. 2020. “Wrist Pain in Gymnasts: Efficacy of a Wrist Brace to Decrease Wrist Pain While Performing Gymnastics.” Journal of Hand Therapy: Official Journal of the American Society of Hand Therapists 33(3): 354–60. https://doi.org/10.1016/j.jht.2019.03.002
- Webb, Brian G., and Lance A. Rettig. 2008. “Gymnastic Wrist Injuries.” Current Sports Medicine Reports 7(5): 289–95. DOI: 10.1249/JSR.0b013e3181870471
- Westermann, Robert W. et al. 2015. “Evaluation of Men’s and Women’s Gymnastics Injuries: A 10-Year Observational Study.” Sports Health 7(2): 161–65. https://doi.org/ 10.1177/1941738114559705
- Seegmiller, D. B., Eggett, D. L., & Charles, S. K. (2016). The effect of common wrist orthoses on the stiffness of wrist rotations. Journal of Rehabilitation Research and Development, 53(6), 1151–1166. https://doi.org/10.1682/JRRD.2014.11.0274
