Abstract:
A management perspective is taken in developing a predictive model to forecast blood oxygen saturation levels for trekkers and mountaineers ascending to high altitudes. Blood oxygen saturation is an important indicator of risk of acute mountain sickness and other potentially lethal health risks for high-altitude athletes. This model is based on data collected from a seventeen-person expedition to Mt. Everest. The results of the model are compared to actual saturation levels and the model is found to be a good predictor. The practical implication is that an oximeter and the results it produces are useful tools for expedition managers and base camp managers charged with the safety of a multi-person expedition.
Introduction:
Mountaineering expeditions can include individuals from varied backgrounds of varied levels of fitness possessing a wide range of technical abilities. They are often led by seasoned climbers and typically involve some external parties who bring needed resources to the table. Such third parties can include university-level researchers, corporate sponsors, or philanthropists who support mountaineering. Regardless of their specific interests, these third parties alter the reality of an expedition, as they have their own objectives and, due to resource contributions, possess considerable influence.
In April 2005, the authors of this paper were part of the core organizing team for a major expedition to Mount Everest – a climbing and research expedition in the Khumbu region of Nepal. The expedition – known officially as the Kanatek Expedition to Mount Everest – involved seventeen individuals, including a mountaineer summit aspirant, several support climbers, sponsors, researchers, research assistants, and trekkers. The unusually diverse nature of the team composition, in terms of goals and objectives, physical fitness, and mountaineering experience, posed many challenges for the management of the expedition.
It was in the course of this expeditionary experience that the importance of physiological measures to the overall management of a large team became clear. A high-altitude mountaineering expedition into remote locations must be self-sufficient in maintaining the health and well-being of participants, and in the logistical supports needed to keep the team moving upwards. In the harsh, highly interdependent, and under-resourced environment that is the Khumbu region, a single expedition member becoming sick may mean the end of a summit bid, the loss of key research time, and overall dissatisfaction and low momentum for the entire team. Yet practical time and cost constraints and ongoing mobility requirements act to limit the availability of information to assist expedition managers in monitoring team performance and managing risks during the ascent.
Typically, the expedition manager faces many complex decision tasks based only on scant information about altitude and weather reports for the team location and planned route, and on the apparent health and acclimatization of the team members. In large expeditions, individualistic and continual assessment of team health is not practical. It therefore is often managed by exception – progress upwards continues unabated unless a team member comes forth with a health complaint. But social pressures may conspire to hide complaints from the expedition manager, as they may entail delays for the rest of the ambitious and highly motivated team. As a result, the exception and the attendant health risk may be apparent only at a late stage, when the feasible range of mitigating actions of the expedition manager may be limited or may entail risks and costs of their own. For example, during our expedition we witnessed a case where a participant of another expedition continued to ascend despite declining health. When the situation was discovered that night, the only response available to that expedition manager was to strap the participant onto a horse obtained from a neighboring village and send the horse down precarious trails into a lower altitude valley during the dark of night. The risks to the participant and the continuing logistical challenges for the expedition manager are both obvious and severe.
It is in response to the challenge of managing team and individual progress in the face of extremely limited management information that we set out to develop a predictive tool for expedition managers – something to assist in the proactive management of health risks for participants and the logistical management of expedition resources and team progression. It is the thesis of this research that the development of a predictive model will provide valuable knowledge and key management information for researchers in mountaineering and for planners and managers of expeditions. Our purpose is to develop a predictive model of physiological acclimatization, based on empirical data from high-altitude sport, suitable for assisting with the management of expeditions into remote alpine regions. More specifically, our objective is to construct a model that can predict blood oxygen saturation based on current altitude and heart rate and on lagged values (i.e., previous values in the time series) of all three indicators.
Literature Review:
The relevant literature for this study stems from two areas: sport management and physiology of acclimatization. Each is briefly presented here.
Sport Management
As with many niche areas of sport management literature (e.g., endurance sport, action sport, etc.), limited attention has been paid to the unique aspects of high-altitude sport (Costa, 2005). Further, although mountaineers are often engaged as subjects in physiology and psychology studies, the literature targeted at developing best practices for the supporting expedition managers and marketers in high-altitude sport is non-existent. General outdoor leisure has received some attention in the literature, in studies often focused on understanding that people take part in outdoor activities seeking to partake in activities that provide ‘personal difference’, given that day-to-day work and life patterns are becoming increasingly similar amongst members of modern society (Bouchet, 1994). As Varley and Crowther point out, climbers involve themselves in outdoor recreation for four basic purposes (Varley and Crowther, 1998): (i) that their roles as participants are congruent with their expected roles as climbers, (ii) that the experience builds towards their future visions of themselves, (iii) performance and (iv) that they are becoming part of a specific community through the shared experiences and rituals that happen. Recently, the literature has evolved to include topics like ecotourism (Herbig and O’Hara, 1997) and action sports (Bennet, Henson et al., 2002). Although mountaineering is not specifically identified in much of this literature, it certainly falls under the scope of such studies.
In considering the best managerial practices for the constrained and challenging environment that is an expedition, the literature provides little direct help. Indirectly, tactics can be drawn from the literature on sport consumer behaviour. Considerable research exists on participation in sporting activities (Kahle, Kambara et al., 1996; McDonald, Milne et al., 2002; Funk, Mahony et al., 2003), although the majority of the literature is based on indirect participation (spectating) as opposed to direct participation. In most cases, the focus is on motivating fan or volunteer attendance at an event (Van Zyl and Botha, 2004). Other studies have called for increased understanding of the sport consumer in lifestyle sports to further explore the participant-spectator relationship (Schouten and McAlexander, 1995; Funk, Mahony et al., 2003).
Acclimatization
Human activity at high altitudes, such as mountaineering and aircraft flight, exposes participants to an environment characterized by many physical hazards – reduced atmospheric pressure, reduced oxygen levels (hypoxia), reduced temperatures, and increased solar radiation. These environmental changes result in many physiological changes in the body, including oxygen consumption, pulmonary ventilation, blood oxygen saturation, blood pressure, and blood chemistry (Basu, Gautam et al., 1996). Of these, hypoxia poses several unique challenges for athletes, those exposed to high altitudes, and those exposed to hypoxia through other mechanisms (sleep apnea, cerebral trauma, etc.) (Wilson, 1996; Sajkov, Marshall et al., 1998).
Hypoxia impacts human physical performance. In a review of studies of high-altitude athletic performance, Fulco et al found that performance of many forms of exercise is impaired, and that this impairment is correlated with altitude. But they also found that this impairment becomes somewhat reduced with prolonged exposure at that altitude (Fulco, Rock et al., 1998). This reduction in negative performance is due to the body acclimatizing to the reduced oxygen levels.
More important than this negative performance impact, continued exposure to high altitude and hypoxia creates serious risks to the health of the individual. Climbers and trekkers may suffer from acute mountain sickness (AMS) or potentially life-threatening edemas. In the case of high-altitude cerebral edema (HACE), elevated blood pressure leads to the transport of blood plasma across the blood/brain barrier. The resulting injury to brain tissue can cause severe discomfort, cognitive impairment, coma, and death in mere hours. In the case of high-altitude pulmonary edema (HAPE), the elevated blood pressure leads to the transport of blood plasma into the aveoli of the lungs. The resulting flooding of lung structures can cause difficulty breathing and eventual death due to drowning in one’s own fluids – again in mere hours (Hackett, 1980; Bezruchka, 1994; Houston, 1998; Dietz, 2005; HRA, 2005; HRA, 2005a).
When exposed to high-altitude hypoxic environments, the body makes several adaptations over time (Houston, 1998; Green, Roy et al., 2001). These acclimatization responses can take many forms. More red blood cells are produced to carry oxygen. The lungs increase in size to facilitate the gaseous exchange of oxygen and carbon dioxide (Cerny, Dempsey et al., 1973). There is also an increase in the vascular network of muscles, which enhances the transfer of gases. But these adaptations are rate delimited. Sudden exposure to high-altitude hypoxic environments, without allowing time for acclimatization, can lead to loss of consciousness in minutes. At 6,000 m, an unacclimatized individual will typically have five to twelve minutes of usable consciousness. At 7,500 m, this time is reduced to three to five minutes. At the Everest summit, only one to two minutes are available (Allstar 2004).
The physical and performance risks of extreme altitude can therefore be managed by controlling one’s rate of ascent. If the ascent is slow enough, the body can sufficiently acclimatize to mitigate these physiological risks. An ascent-rate heuristic adopted by many trekkers, and recommended by the Himalayan Rescue Association (HRA), is to gain no more that 300m altitude in a single day (Dietz, 2005; HRA, 2005). Any days where the altitude gain exceeds this should be followed by a rest day in which the trekkers gain no additional altitude. During this rest day, the body can further acclimatize and the individual can be monitored for early symptoms of detrimental health issues.
The Expedition:
In April 2005, the authors participated in a research expedition to the Khumbu region of Nepal, including a trek to the base camp of Mt. Everest and an ascent of the mountain itself. This expedition was an interdisciplinary endeavour that brought together researchers and support personnel from four countries to share in the objective of obtaining data for thirteen diverse research projects. These projects ranged from tourism management studies based in the tourist areas of Kathmandu, to physiological and psychological studies conducted at high altitudes on Mt. Everest.
The journey from Kathmandu to Everest base camp involves a forty-five minute flight to Lukla airstrip (altitude 2840m), followed by a ten-day trek up to base camp (5400m). Figure 1 shows the altitude of the expedition team during this multi-day ascent, as well as the names of the various towns and villages where overnight camps were established. The long plateaus at Namche (3440m) and Dingboche (4410m) reflect the rest days that were included. These rest days allowed additional time for physiological acclimatization after unusually large altitude gains on the previous days.
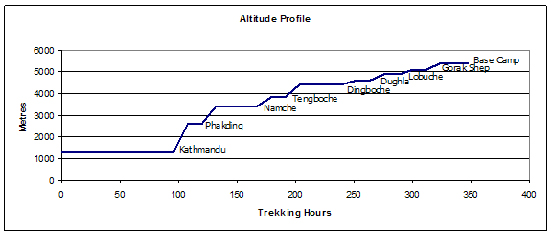
Figure 1: Altitude Profile
In addition to adherence to the HRA heuristic for altitude gain, the expedition team monitored the oxygenation of blood for all members during the ascent. Any members who displayed a significant drop in oxygen saturation, despite not exhibiting symptoms of AMS, would be required to remain at the current altitude for an additional rest day with a support crew, and would rejoin the main expedition later at base camp. The regular and periodic monitoring of blood oxygen saturation levels was, therefore, an established protocol for the expedition, separate from the use of such data for the current study.
Methodology:
Participants in this study comprised the seventeen members of the research team, which had three women and fourteen men, ranging in age from 22 to 63. The range of physical fitness and outdoor recreational activity for these participants varied widely, with some subjects being multiple participants in triathlons and “Iron Man” competitions or being experienced mountaineers, and other subjects coming from thirty years of sedentary office jobs and having never before hiked in strenuous terrain. These less-active subjects had participated in a six-month training program prior to the expedition, which included weekly 300-floor stair climbs in the office towers of downtown Toronto. Eight of the participants had no prior experience of being at very high altitudes of over 3,700 metres (Curtis 1995); only two had been at such altitudes on more than two prior occasions.
Three measures were collected: altitude, resting heart rate, and SpO2 peripheral blood oxygen saturation level. Altitude was measured by reference to a topographic map (NGS, 2000), where current location was assessed by experienced trekkers on the expedition team, including one professional geographer. This altitude measurement was further validated by comparison to barometric altitude readings obtained from wristwatch devices carried by two other expedition members.
Heart rate and saturation were measured by use of a Nonin 9500 Onyx digital finger pulse oximeter. This oximeter is small and inexpensive, making it a feasible addition to the equipage for a mountaineering expedition manager. The non-invasive device is applied to a fingertip, and uses the transmission of light from an LED through the finger tissue to determine pulse and blood oxygen levels. Blood oxygen level is inferred by a spectroscopic analysis of the light transmission; simply put, oxygenated blood is a different color, and this difference can be observed by the device. After a short delay, measures of heart rate and saturation are displayed by the device on a numeric display. Such oximetry devices have a long history of use in physiological research and for high-altitude health monitoring (Wong, 1945; Powers, Dodd et al., 1989; Fearnley, 1995; O’Connor, Dubowitz et al., 2004).
Two precautionary protocols were observed for all readings to improve the reliability of the device readings. First, to account for differing levels of prior activity, each subject must have been sitting and resting for at least fifteen minutes prior to reading the heart rate. Secondly, fingertips must have been at normal surface body temperature, to prevent artificially lower saturation readings due to vasoconstriction in cold fingers (Powers, Dodd et al., 1989; Awad, Ghobashy et al., 2001). This became progressively more challenging as we ascended to higher and colder altitudes, so steps were taken ensure fingertips were at normal body temperatures before readings. The quality and quantity of data collection was unchanged as the expedition progressed higher.
These data were collected twice daily from each participant: immediately before breakfast and immediately before dinner (typically 6:00 a.m. and 7:00 p.m. respectively). At these times, all expedition members were gathered together, and would have had similar prior activity levels (e.g., general light activity around camp). Data were recorded electronically on a handheld PDA device and were later converted to an Excel file on a PC. Figure 2 shows the average blood saturation level for the team over the course of the ascent to Everest base camp, while figure 3 shows the corresponding average resting heart rate.
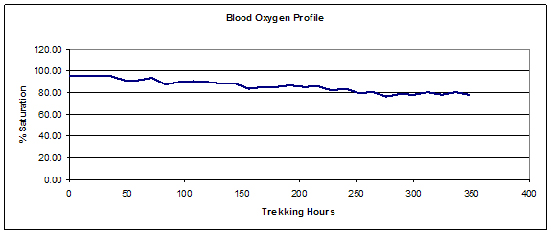
Figure 2: Blood Oxygen Profile
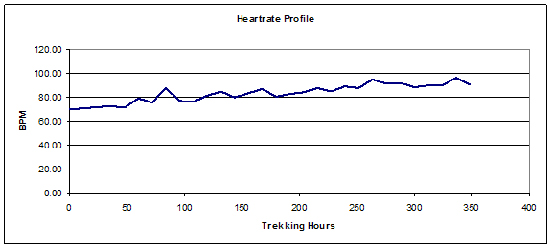
Figure 3: Heart Rate Profile
Analysis:
The data were imported into SPSS (version 12.0) for analysis and model-building, via ordinary least squares linear regression.
Since the expedition group remained together for the duration of the ten-day ascent, the same altitude measures were ascribed to all members each day. Blood saturation and heart rate measures were individually recorded, and were subsequently averaged for the group. Checks for heteroskedacity of these measures were performed through visual inspection of the superimposed individual trend graphs.
A number of simple data transformations were made prior to modeling attempts. The altitude profile of figure 1 was made linear by squaring the data. The non-stationary trend data for all three variables was made stationary by first-differencing. The resulting stationary data was checked for normality using the Kolmogorov-Smirnov test (Kolmogorov 1941).
The modified data was then used to construct a vector auto-regression predictive model (Cooley and LeRoy, 1981; Pagan, 1987; Pagan, 1995). Vector auto-regression is an atheoretical approach to predictive modeling that makes no restrictive a priori assumptions about which independent variables may account for variance in the dependent variables. Rather, it assumes that all variables may have influence on all other variables, and therefore a vector of all variables is auto-regressed to lagged values of the same vector.
| Model | Unstandardized Coefficients |
Standardized Coefficients |
t | ρ | ||
| B | SE | Beta | ||||
| Constant | -.436 | .803 | -.543 | .595 | ||
| ASD2 | .241 | .260 | .175 | .928 | .367 | |
| SD2 | -.594 | .218 | -.618 | -2.723 | .015 | |
| SD3 | .084 | .268 | .086 | .313 | .758 | |
| HD2 | -.184 | .109 | -.375 | -1.682 | .112 | |
| .224 | .234 | .162 | .957 | .353 | ||
| HD1 | -.240 | .097 | -.506 | -2.472 | .025 | |
| ASD3 | -.435 | .236 | -.315 | -1.846 | .083 | |
| HD3 | -.071 | .095 | -.141 | -.745 | .467 |
Variables:
SD1 – Dependent variables; saturation difference, current period
SD2 – Saturation difference, one period previous
SD3 – Saturation difference, two periods previous
HD1 – Heart rate difference, current period
HD2 – Heart rate difference, one period previous
HD3 – Heart rate difference, two periods previous
ASD1 – Altitude squared difference, current period
ASD2 – Altitude squared difference, one period previous
ASD3 – Altitude squared difference, two periods previous
Although vector auto-regression is an atheoretical approach, we allowed theoretical considerations to inform our choice of lags to include in the model. Both heart rate and saturation are physiological responses to increases in altitude and are subject to acclimatization of the body (Dietz, 2005; HRA, 2005). Full acclimatization can take several days, but for trekkers who make occasional gains in excess of 300m, substantive improvements in acclimatization can be achieved by resting at current altitude for twenty-four hours (Dietz 2005). For this reason, we included lagged variables for the two previous semi-daily readings (i.e., twelve hours prior and twenty-four hours prior). In effect, we created a regression model in which blood oxygen saturation level is predicted by previous values of saturation, heart rate, and altitude. The regression results for this model are presented in table 1, showing both standardized and unstandardized regression coefficients, as well as significance levels. This regression yielded an R2 of 0.706, indicating that high proportion of the variation in observed saturation levels can be accounted for and predicted by the independent variables of the model. The model is overall significant at ρ = 0.044 despite the low significance of some of the individual coefficients (see table 1), reflecting a multicollinearity common to vector autoregression models. In equation form, the model of table 1 can be represented as:
SD1 = – 0.618*SD2 + 0.086*SD3 – 0.506*HD1 – 0.375*HD2 – 0.141*HD3 + 0.162*ASD1 + 0.175*ASD2 – 0.315*ASD3 + error
Or, in terms of the measured variables without transformation:
St = St-1 – 0.618*(St-1 – St-2) + 0.086*(St-2 – St-3) – 0.506*(Ht – Ht-1) – 0.375*(Ht-1 – Ht-2) – 0.141*(Ht-2 – Ht-3) + 0.162*(At*At – At-1*At-1) + 0.175*(At-1*At-1 – At-2*At-2) – 0.315*(At-2*At-2 – At-3*At-3) + error
Where Si is saturation (%) at time i
Hi is heart rate (bpm) at time i
Ai is altitude (m) at time i
Vector autoregression is an atheoretical approach, so caution should be used in interpreting these results. Large and significant coefficients do not necessarily suggest causal relationships; they suggest relationships of high predictive validity only. In the case of the current model, the results suggest that blood oxygen saturation can be meaningfully predicted from historical saturation levels, as well as the recent profile of altitude gain and resting heart rates. The largest predictive factors are the twelve-hour changes in saturation level and heart rate, and the twenty-four hour changes in heart rate.
The regression model based on standardized coefficients was initially tested by using it to forecast the average group saturation data shown in figure 2. Figure 4 compares of the actual and forecasted saturation levels for the twenty-five forecastable measurement points (two initial points are lost due to differencing).
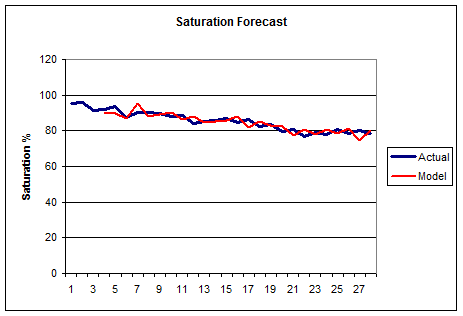
Figure 4: Model Aggregate Forecast Performance
The fit of the model to the actual observed data appears very good, but may be benefiting from regression to the mean. Of greater practical importance to expedition managers would be the model’s ability to accurately predict saturation levels for individuals. Figure 5 shows the same model applied to individual data for three of the participants. The predictive ability of the model still appears to be good.
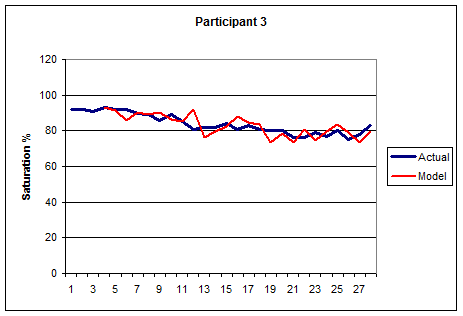
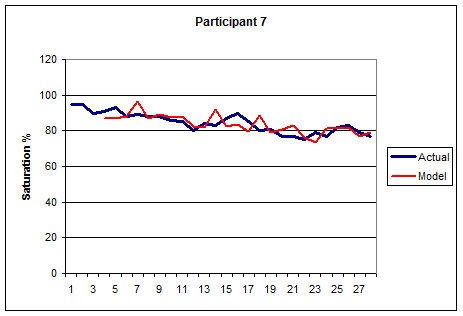
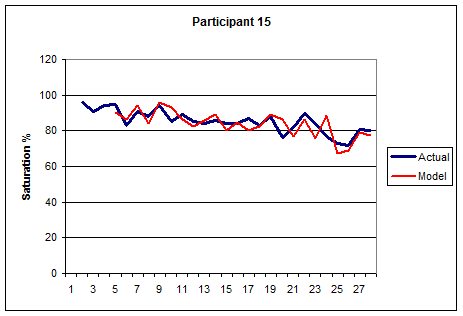
Figure 5: Individual Forecast Performance
Discussion:
The safety of sports recreation and sports management at high altitudes remains a challenge, especially for inherently high-risk sports such as mountaineering. The objective hazards of the alpine environment are exacerbated by subjective hazards due to choices made in climbing practices. Of these, the rate of ascent and time allowed for acclimatization are especially important, as the dangers of AMS and high-altitude edemas are ever-present and potentially very serious. To the extent that the present model can be used to make first-order estimates of expected blood oxygen saturation, it may be helpful to trekkers, climbers, and others who manage travel to high altitudes. With its limitations, the present study has yielded a model that provides a fairly good ability to make such forecasts, and might prove useful as one of many tools in a complete program of mountain safety precautions.
The development of such a model provides expedition managers with a simple and practical tool to monitor and assess the performance of teams involved in high-altitude sport activities. It provides managers with an additional tool to predict performance and acclimatization of teams and individuals and to assess their teams and prevent major issues with AMS as an ‘early warning system’. To illustrate with a specific example, we refer to the case of Participant 15 shown in figure 5. Had the present model been available to the manager of this expedition, it would have provided guidance for the proactive monitoring of this participant, and for decision-making with respect to the rate of progress for the entire expedition team. First, the model highlights a rapid decline in saturation during Periods 24 and 25, indicating a need for close medical monitoring for signs of deteriorating performance or growing safety risks. A prolonged drop in saturation could have necessitated a halt to the progress of the expedition team up the mountain, or even resulted in sending this individual and a support team down to lower altitudes to recover. Either of these scenarios would have entailed significant costs and logistical challenges for the expedition manager. Augmented with data for the next day, the model subsequently predicts a recovery of the individual saturation level to 80% by the following day, suggesting that the continuation of the team ascent was still a feasible option for the expedition manager. In both cases, the subsequent acclimatization of the individual unfolded as the model predicted. But, absent the model, the expedition manager faced a much more difficult risk management challenge.
These results, although certainly limited, suggest that an oximeter and twice-daily data analysis are useful in determining the adaptation levels of all team members and in making decisions about rate of team progress and the close monitoring of individuals. The larger the team managed, the more helpful the tool is likely to be, as regular and direct observation of all individual team members becomes more difficult in larger expeditions. Although more research is certainly required in the area, the authors feel that this study shows evidence of how science and technology can support management in a highly constrained sports environment, and they plan to continue their work in the area.
Limitations:
The generalizability of this model from a data analysis point of view may be limited by the variation and representativeness of the subjects that were included. While the sample exhibited significant variation in ages, fitness levels, and prior experience, it was less variable in other factors, such as gender and ethnicity. The variables included in the model were single-item measures, which raises potential reliability concerns. Moreover, validity concerns can be raised related to the control of variables that were not measured or included in the model. In particular, the depth of ventilation during or immediately prior to oximetry measurement, including the possibility of hyperventilation (either conscious or unconscious), may impact the reliability of heart rate and saturation measures. Furthermore, to the extent that conscious changes in breathing patterns may influence oximetry readings, the threat of social desirability bias also appears. Since a low saturation score carried the implied threat of being left behind by the main group, participants may have had incentive to attempt to inflate their saturation scores.
Acknowledgements:
This study is dedicated to the memory of Dr. Sean Egan, an expedition team member who tragically perished on the slopes of Mt. Everest during his bid to reach the summit. Dr. Egan was a fine researcher, an accomplished climber, and an excellent human being who inspired us all.
References:
Allstar (2004). Altitude and oxygen. F. I. University, http://www.allstar.fiu.edu/aero/oxygen.htm
Awad, A.A., Ghobashy, A.M., et al. (2001). “Different responses of ear and finger pulse oximeter wave form to cold pressor test.” Anesthesia & Analgesia 92(6): 1483-1486.
Basu, C.K., Gautam, R.K., et al. (1996). “Metabolic responses during initial days of altitude acclimatization in the Eastern Himalayas.” International Journal of Biometeorology 39(3): 133-138.
Bennet, G., Henson, R., et al. (2002). “Action sports sponsorship recognition.” Sport Marketing Quarterly 11(2): 174-185.
Bezruchka, S. (1994). Altitude illness: Prevention & treatment. Leicester UK, Cordee.
Bouchet, D. (1994). “Rails without ties:The social imaginary and post modern culture. Can postmodern consumption replace modern questioning?” International Journal of Marketing 11: 405-422.
Cerny, F.C., Dempsey, J.A., et al. (1973). “Pulmonary gas exchange in non-native residents of high altitude.” Journal of Clinical Investigation 52: 2993-2999.
Cooley, T.F. and LeRoy, S.F. (1981). “Identification and estimation of money demand.” American Economic Review 71: 825-844.
Costa, C.A. (2005). “The status and future of sport management: A Delphi study.” Journal of Sport Management 19(2): 117-142.
Curtis, R. (1995). Outdoor Action guide to high altitude: Acclimatization and illnesses. Princeton NJ, Outdoor Action Program.
Dietz, T.E. (2005). An altitude tutorial. International Society for Mountain Medicine, http://www.ismmed.org/np_altitude_tutorial.htm
Fearnley, S.J. (1995). “Pulse oximetry.” Practical Procedures 5(2): 1.
Fulco, C.S., Rock, P.B., et al. (1998). “Maximal and submaximal exercise performance at altitude.” Aviation, Space, and Environmental Medicine 69(8): 793-801.
Funk, D.C., Mahony, D.F., et al. (2003). “Sport consumer behaviour: Assessment and direction.” Sport Marketing Quarterly 12(4): 200-205.
Green, H.J., Roy, B., et al. (2001). “Efficiency after altitude acclimatization.” Journal of Applied Physiology 91: 1014-1015.
Hackett, P.H. (1980). Mountain sickness: Prevention, recognition, treatment. New York NY, American Alpine Club.
Herbig, P. and O’Hara, B. (1997). “Ecotourism: A guide for marketers.” European Business Review 97(5): 231-236.
Houston, C. (1998). Going higher: Oxygen, man and mountains. Seattle WA, The Mountaineers.
HRA, H. R. A. (2005). Altitude, http://www.himalayanrescue.org/hra/altitude.php
HRA, H. R. A. (2005a). Altitude Sickness, http://www.himalayanrescue.org/hra/altitude_sickness.php
Kahle, L., Kambara, K., et al. (1996). “A functional model of fan attendance motivations for college football.” Sport Marketing Quarterly 4: 51-60.
Kolmogorov, A. (1941). “Confidence limits for an unknown distribution function.” Annals of Mathematical Statistics 12: 461-463.
McDonald, M. A., Milne, G.R., et al. (2002). “Motivational factors for evaluating sport spectator and participant markets.” Sport Marketing Quarterly 11: 100-113.
NGS, N. G. S. (2000). Everest base camp. National geographic trails illustrated: Adventure map.
O’Connor, T., Dubowitz, G., et al. (2004). “Pulse oximetry in the diagnosis of acute mountain sickness.” High Altitude Medicine & Biology 5(3): 341-348.
Pagan, A. R. (1987). “Three econometric methodologies: A critical appraisal.” Journal of Economic Surveys 1: 3-24.
Pagan, A. R. (1995). Three econometric methodologies: An update. Surveys in Econometrics. L. Oxley. New York NY, Marcel Dekker: 605-618.
Powers, S. K., Dodd, S., et al. (1989). “Accuracy of pulse oximetry to estimate HbO2 fraction of total Hb during exercise.” Journal of Applied Physiology 67: 300- 304.
Sajkov, D., Marshall, R., et al. (1998). “Sleep apnea related hypoxia is associated with cognitive disturbances in patients with tetraplegia.” Spinal Cord 36(4): 231-239.
Schouten, J. W. and McAlexander, J.H. (1995). “Subcultures of consumption: An ethnography of the new bikers.” Journal of Consumer Research 22: 43-61.
Van Zyl, C. and Botha, C. (2004). “Motivational factors of local residents to attend the Aardklop National Arts Festival.” Event Management 8(4): 213-222.
Varley, P. and Crowther, G. (1998). “Performance and the service encounter: An exploration of narrative expectations and relationship management in the outdoor leisure market.” Marketing Intelligence & Planning 16(5): 311-317.
Wilson, B. (1996). “Cognitive functioning of adult survivors of cerebral hypoxia.” Brain Injury 10(12): 863-874.
Wong, Y. T. (1945). “The measurement of blood oxygen in malaria with the use of the oximeter.” Science 102(2646): 278-279.
