Authors: Jack Clarke, Lynn Allen
Department of Sport and Health Sciences, Athlone Institute of Technology, Westmeath, Ireland
Corresponding Author:
Jack Clarke
An Luslann, Kylebroughlan, Moycullen,
Co. Galway, H91 TXV5, Ireland.
Email: jackclarke199@gmail.com
Mr. Jack Clarke is a recent graduate of Athletic and Rehabilitation Therapy at Athlone Institute of Technology, Ireland. He is currently furthering his studies at Loughborough University, United Kingdom. His professional interests circulate around athletic performance development, strength and conditioning, and musculoskeletal therapeutic interventions particularly in track and field events.
Ms. Lynn Allen is a Certified Athletic Therapist currently in the role of lecturer and course coordinator of Athletic and Rehabilitation Therapy at Athlone Institute of Technology, Ireland. Her professional interests include athletic therapy clinical education, biopsychosocial framework for chronic pain and athletic injuries, clinical education curriculums, and musculoskeletal therapeutic interventions.
The effects of muscle energy techniques on latent trigger points of the gastrocnemius muscle
ABSTRACT
Purpose: The purpose of this study is to examine the effectiveness of muscle energy technique post isometric relaxation as a treatment method for latent trigger points within the gastrocnemius muscle. This study also compares the muscle energy technique post isometric relaxation to ischemic compression to determine the most effective latent trigger point treatment. The outcome aim is to understand the acute and mid-term effects of the treatment and how the results may apply to an athletic therapy population.
Methods: 40 participants (24 male and 16 female) were randomly assigned to two treatment groups that took part in three treatment sessions over the course of 10 days. Group A took part in a muscle energy technique post isometric relaxation protocol and Group B took part in an ischemic compression protocol.
Results: There was a statistically significant treatment effect in both groups for both the reduction of latent trigger point numbers (p<.0005) and increasing ankle dorsiflexion range of motion (p<.0005). The muscle energy technique treatment was more effective than the ischemic compression treatment in latent trigger point reduction and increasing range of motion (p=0.26, p=0.58 respectively).
Conclusions: This study concludes that both muscle energy technique post isometric relaxation and ischemic compression effectively treat latent trigger points in the gastrocnemius following acute and mid-term treatment. Muscle energy technique post isometric relaxation is more effective than ischemic compression indicating that muscle energy technique post isometric relaxation is the most effective form of treatment for latent trigger points found in the gastrocnemius.
Applications in Sport: Athletic therapists and sport related clinicians are recommended to use muscle energy technique post isometric relaxation in situations where latent trigger points are found within the gastrocnemius.Muscle energy technique post isometric relaxation is a suitable treatment method to use in a variety of settings that an athletic therapist or clinician may be in, such as pre-game and post-game therapy, on-field therapy, and clinical therapy
Keywords: Trigger point, METs, MET PIR, post isometric relaxation, muscle therapy, lower limb
INTRODUCTION
A trigger point (TrP) is a discrete, focal, hyperirritable point in a taut band of skeletal muscle (5). TrPs develop in muscles because of myofascial or overuse injuries (24). Athletes participating in competitive sports such as athletics, rugby union, basketball, and soccer, are predisposed to overloading the muscle and creating the TrPs. The TrPs create a constant shortening within the effected muscle (2,25) causes disruption to the muscle’s normal functionality, predisposing the individual to injury (18,23). There are two forms of TrP: active and latent. Both forms of TrP are characterized by their physical characteristics (1,12). Active TrPs (ATrPs) cause muscle dysfunction, referred pain and tenderness in a muscle during times of stress or activity (2,24). Latent trigger points (LTrPs) do not produce pain during times of stress or activity however they do cause muscle dysfunction (2,18,24).
This study is focused on LTrPs found within the gastrocnemius. Previous research articles investigating TrPs have not focused on LTrPs in solidarity, so the current knowledge is unspecific. It is known however that both ATrPs and LTrPs can be reduced using invasive and non-invasive treatment modalities (6,7,10). There are a wide range of treatments that have suggested positive results however the research has not always been supported with consistent results.
An interesting non-invasive treatment that has shown promise with reliable studies is the muscle energy technique (MET). METs are a manual technique involving the muscles own energy to lengthen the muscle fibres and remove the sustained contractions that cause the TrP (3,19). It is theorized that METs mechanically uncouple the myosin and break the energy crisis cycle (4). METs have shown promising effects in the removal of TrPs (11,16,21-22,). However, the current understanding surrounding METs has specifically been tested on ATrPs within the upper trapezius. The current understanding of METs implies that METs are a reliable and effective method for TrP treatment. However, the research has not extensively investigated LTrPs and lacks research studying a variety of muscles. MET research also lacks consistency in research protocol design. MET has become an umbrella term for non-invasive treatment techniques utilizing muscle energy to lengthen muscle fibers, but no clear protocol has been followed. The most consistent MET treatment protocol to date is the method of post isometric relaxation (PIR). MET PIR has been investigated by a number of studies focused on ATrPs in the upper trapezius (8,13-15,26). This research study investigates the application of MET PIR on LTrPs within the gastrocnemius muscle.
This study’s research hypothesis and primary aim is to investigate the ability of MET PIR at reducing the presence of LTrPs in the gastrocnemius, a previously unexplored area. The secondary aim of this study is to expand the knowledge of METs and their effect on LTrPs by forming a comparison with the previously effective treatment, ischemic compression (IC). The study will compare the effect of the MET PIR method against IC following acute and mid-term treatment protocols.
The study’s first objective is to assess the ability of each treatment in removing the LTrP. The second objective is to assess the compressive sensitivity of the LTrP following treatment. Finally, this study’s third objective is to assess the ability of each treatment to restore normal muscle function by measuring ankle dorsiflexion range of motion (ROM). The potential application of this study is to reduce the exposure of injuries caused by LTrPs in the athletic population competing in lower limb impact sports.
METHOD
Participants
This study utilized a quasi-experimental comparative study to measure the acute and mid-term treatment effect of MET PIR. This study utilized data from 40 trained athletes (24 males, 16 females) participating in lower limb impact sports (age = 21.18 ± 1.18 years, training sessions per week = 3.15 ± 0.94 sessions, hours training per week = 4.6 ± 1.38 hours).
Procedures
Three independent variables were chosen to measure any treatment effect: the number of LTrPs present, LTrP compressive-sensitivity and active ankle dorsiflexion range of motion. Measurements from the MET PIR treatment protocol was compared to the IC treatment protocol.
Participants were randomly divided into two treatment groups; group A and group B. Treatment group A (male=11, female=9) followed a MET PIR treatment protocol. Treatment group B (male=13, female=7) followed an IC treatment protocol. Both groups participated in three treatment protocols over 10 days carried out on their dominant leg. Each treatment protocol was carried out by the same therapist throughout the entire study to exclude inter-rater variability. Prior to each treatment session all participants, irrespective of group, took part in pre-protocol testing which measured active ankle dorsiflexion and the total number of LTrPs present within the gastrocnemius which followed Simons et al.’s (24) TrP identification criteria. Following each treatment session each participant was re-examined to detect any acute change. This study measured a total of four points that could be used to measure treatment progression throughout the protocol; baseline measurements (BL) taken before treatment began, post session one measurements (S1), post session two measurements (S2) and post session three measurements (S3).
Group A participants followed a MET PIR protocol that has been commonly used throughout MET PIR research (8, 13-15,26). Participants were positioned prone on a therapy bed with both feet hanging off the bed. The dominant foot was passively pushed into dorsiflexion until a barrier of tension was felt by the participant. The participant was then instructed to contract against the therapist’s resistance for seven seconds with 20% of their maximum strength to create an isometric contraction. After seven seconds, the participant was instructed to relax while the therapist moved their ankle into a deeper range of dorsiflexion until the next barrier of tension was felt. This barrier of tension was held for 60 seconds. This process was repeated three times in total.
Group B participants underwent an ischemic compression treatment protocol outlined by Simons et al. (25). The participants were positioned prone on a therapy bed with both feet positioned off the bed. A LTrP was identified and a gradual pressure was applied until the participant felt a 7/10 level of discomfort on the visual analogue scale. This pressure was held on the LTrP for 30 seconds. The participant was instructed to remain as relaxed as possible throughout this process while breathing deeply at a constant rate. This process was repeated for three repetitions, each round compressing on a different LTrP. Following each treatment protocol both groups were reassessed in ankle dorsiflexion range of motion and LTrP presence and sensitivity using the same testing methods.
Data Analyses
Statistical analyses were performed using SPSS 25. A descriptive analysis was conducted on all collected data groups measuring the mean, standard deviation, 95% confidence interval of all data. A Shapiro Wilke’s for normality was completed on all data to meet the assumptions for the following tests. A two-way mixed analysis of variance (MANOVA) was conducted during the analysis of the two dependent variables: LTrP presence in the gastrocnemius and ankle dorsiflexion ROM. The primary goal of the two-way MANOVA was to explore the effects of both independent variables and compare any differences that may exist between treatment groups. An independent-samples t-test was conducted on the acute and mid-term number of occasions of sensitivity reductions reported in both groups. The primary goal of the independent-samples t-test was to measure the difference between the means each treatment group. It also determined whether the difference was statistically significant.
RESULTS
The data recorded from the four time points throughout the treatment protocol allowed for acute and mid-term measures. Acute effects measured the difference between BL and S1 results. Mid-term effects measured the difference between BL and S3 results.
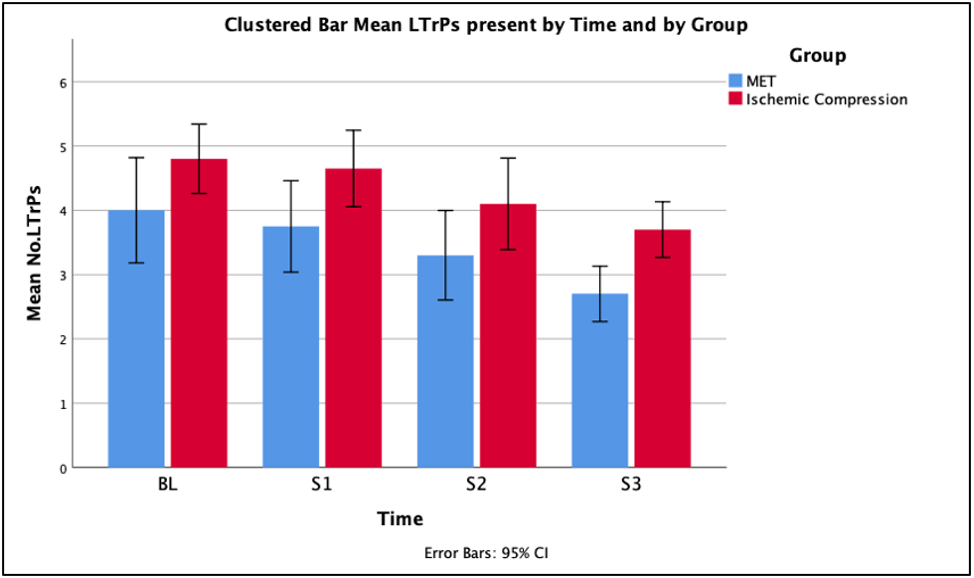
A two-way mixed ANOVA (MANOVA) was conducted to measure the treatment effect on the number of LTrPs in the gastrocnemius. The treatment effect of both treatments on LTrPs present over time can be seen in Figure 1. There was no statistically significant interaction between the intervention and time on the number of LTrPs, F (2.304, 87.555) =.834, p=.452, partial η2= .021. The main effect of time showed a statistically significant difference in the mean number of LTrPs across the different time points, F (3, 114) = 32.349, p< .0005, partial η2 = .460. All participants had an acute mean decrease of 0.3 LTrPs (95% CI, .080 to .520), a statistically significant difference, p<.005. All participants had a mid-term mean decrease of 1.325 LTrPs (95% CI, .892 to .1.758), a statistically significant difference, p< .0005. The main effect of group showed that there was a statistically significant difference in mean number of LTrPs present between both treatment groups, MET and IC, F (1, 38) = 5.340, p=.026, partial η2= .123. The MET treatment had a greater impact on the number of LTrPs present than the IC treatment, with a mean difference of 0.862 LTrPs (95% CI, -1.618 to -.107) with a significant difference at the .05 level.
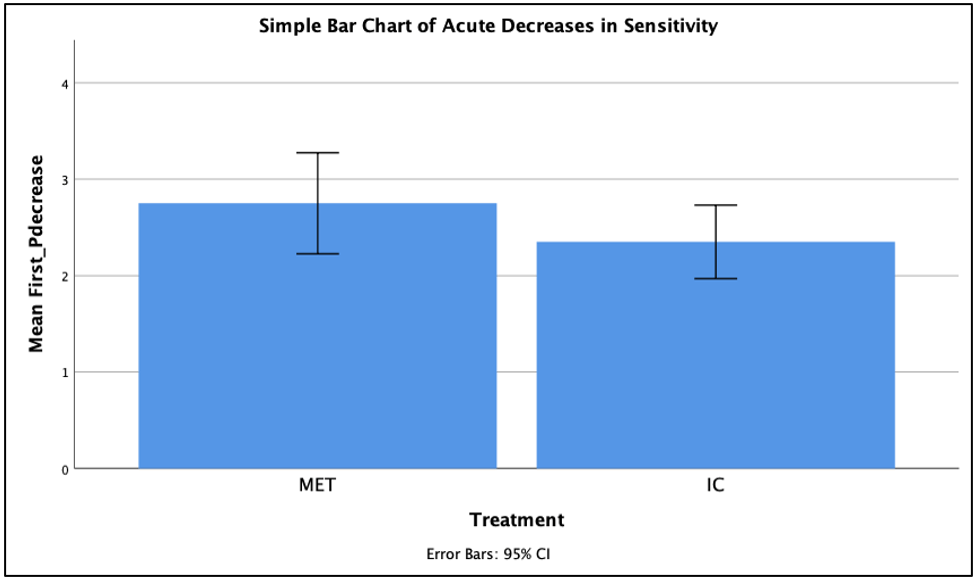
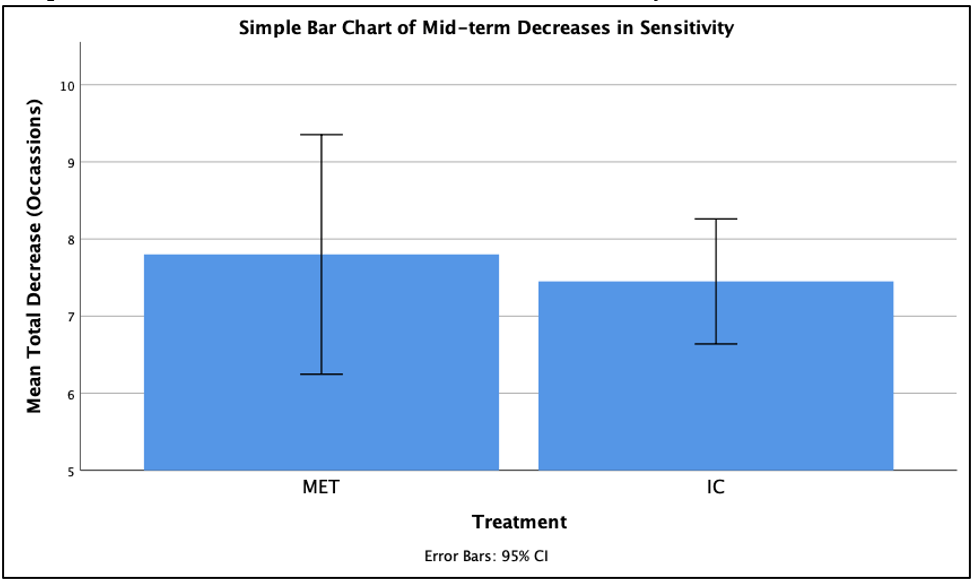
An independent-samples t-test was conducted on the total number of occasions of sensitivity reductions reported after an acute bout of treatment and after a mid-term treatment protocol for both groups. The acute and mid-term decreases in LTrP sensitivity are presented in Figure 2 and Figure 3 respectively. There were more cases of acute sensitivity reduction in the MET treatment group (2.75 ± 1.118) compared to the IC treatment group (2.35 ± .813). The mean difference was 0.4 (95% CI, -0.226 to 1.026). There was no statistically significant difference in acute sensitivity reduction occasions between MET treatment and IC treatment, t (38) =1.294, p>0.5. There were more cases of mid-term sensitivity reduction in the MET group (7.8 ± 3.318) compared to the IC treatment (7.45 ± 1.731). The mean difference between groups was .35 (95% CI, -1.363 to 2.063). There was no statistically significant difference in sensitivity reduction occasions found between treatment groups after three treatment sessions, t(28.631)=.418, p>0.5.
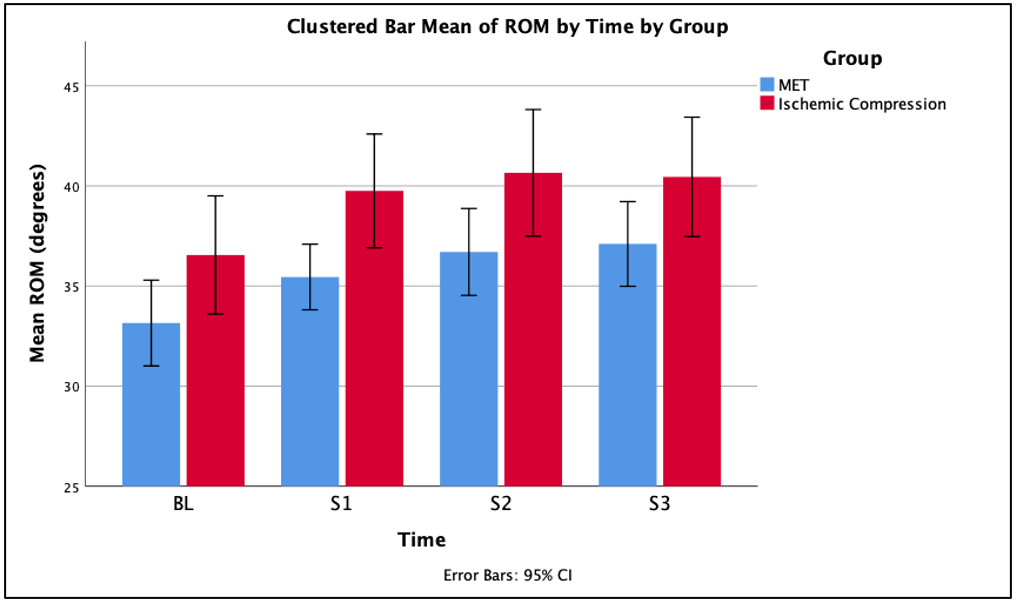
A two-way MANOVA was conducted to compare the dependent variables, MET treatment and IC treatment, in their ability to increase ankle dorsiflexion ROM in the gastrocnemius across four time points. The treatment effect of both treatments on ankle dorsiflexion range of motion over time can be seen in Figure 4. There was no statistically significant interaction between the intervention and time on the ankle dorsiflexion ROM, F (3, 114) =.139, p=.936, partial η2= .004. The main effect of time showed a statistically significant difference in mean ROM across the different time points, F (3, 114) = 34.271, p < .0005, partial η2= .474. All participants had an acute mean increase in ROM with a significant difference. All participants had a mid-term mean increase in ROM with a significant difference. The main effect of group showed that there was a statistically significant difference in mean ROM increase between treatment protocols, F (1, 38) = 3.834, p=.058, partial η2= .092. The MET treatment had a greater increase in ROM than the IC with a statistically significant difference, p=0.058.
DISCUSSION
The purpose of this research was to determine the effectiveness of MET PIR in treating LTrPs within the gastrocnemius muscle while comparing it to IC. To date there has been no research exploring the effects of METs on LTrPs in the gastrocnemius. The application of MET PIR and IC on LTrPs within the gastrocnemius had significant treatment effects following acute and mid-term treatment. The results found that both treatments effectively treat LTrPs and increase the ankle joint dorsiflexion. Furthermore, the MET PIR treatment was significantly more effective that the IC treatment over acute and mid-term treatment.
Effect on LTrP Treatment
The results demonstrated that both treatment protocols had a statistically significant effect on reducing the number of LTrPs across all time points (p<.0005). Both treatments had a statistically significant acute decrease in the number of LTrPs present (p<.005) however the acute mean decrease was 0.3 LTrPs, which is not a clinically significant result. The results do not suggest that MET PIR and IC can immediately remove LTrPs. However, the mid-term effects of both treatment protocols had a statistically significant mean decrease of 1.3 LTrPs (p< .005) (95% CI, .892 to .1.758) suggesting that both treatments are more effective following mid-term treatment. This result is in agreement with Gilani, et al. (11) and Esparaza et al. (9) that both the MET PIR and IC groups had a greater midterm treatment effect compared to one acute bout of treatment. When both treatment groups were compared against each other the results concluded that the MET treatment protocol is significantly more effective at reducing the number of LTrPs within the gastrocnemius than the IC treatment (p=.026), with a mean difference of 0.862 LTrPs. This is finding is in agreement with previous studies from Kumar, et al. (16), Nambi, et al. (21) and Gilani, et al. (11) who also found a MET treatment to be more effective than an IC treatment in the removal of TrPs.
The results of this study demonstrated a significant reduction in LTrP sensitivity following acute and mid-term treatment in both treatment groups. There were more cases of acute and mid-term sensitivity reduction in the MET treatment group however the independent-samples t-test did not measure a statistically significant difference between the groups. This indicates there was no significant difference between the two treatments in their abilities to reduce LTrP sensitivity. The reductions in LTrP sensitivity as a result of MET PIR treatment has been hypothesized by Mahajan, et al. (19) to be the hypoalgesic effects of the inhibitory Golgi tendon reflex, activated during the isometric contraction, leading to reflex relaxation of the muscle. This is evident in this study by the significant reduction in LTrP sensitivity found in the MET PIR treatment group however the study is inconclusive whether the MET PIR treatment was more effective at reducing LTrP compressive sensitivity than IC. Gilani, et al. (11) found similar significant sensitivity reductions following both treatments however they did find evidence to suggest that IC is a more effective method at reducing compressive sensitivity. Similarly, Kumar, et al. (16) also found IC to be more effective in reducing sensitivity after an acute bout of treatment but the MET treatment was more effective at reducing sensitivity over time.
Effect on ankle dorsiflexion range of motion
The results of this study demonstrated that both the MET PIR and IC protocol had a statistically significant treatment effect on ankle dorsiflexion ROM, over acute and midterm treatment (p<.0005). When both groups were compared to each other, the MET PIR treatment had a greater effect on ankle dorsiflexion ROM than IC (p=.058). The findings within this study are in agreement with previous research. Gilani, et al. (11) and Nambi et al. (21) also found that MET treatment is more effective in restoring joint ROM that IC by a significant margin following acute and mid-term treatment. Mahajan, et al.(2012) attributes the superior extending capabilities of METs to physiological mechanisms that adapt the muscles extensibility capabilities. The results taken from this study and the previous studies mentioned demonstrate this theory.
Based on this study, MET PIR is an effective form of treatment for LTrPs in the gastrocnemius. The results suggest that the MET PIR treatment is more effective than IC in the reduction of LTrPs acutely and over mid-term treatment. This study accepts the research hypothesis that MET PIR reduces the presence of LTrPs in the gastrocnemius muscle of athletes participating in lower limb impact sports.
Limitation within the study
A noticeable limitation within this study is that the MET PIR treatment had the ability to treat more LTrPs per session than the IC treatment. The IC treatment protocol was designed to match the same work input as the MET PIR protocol which included three repetitions per session. This limited the amount of LTrPs that had the potential to be treated in the IC group. Future research could explore comparing these treatments using treatment protocols tailored to each treatment individually. The sample size of this study was also a limitation that restricted statistical analysis. The two-way MANOVA test used in this study is not a robust test and is most effective with higher sample sizes. Future research replicating this study should study a greater sample size.
CONCLUSION
This study reveals that MET PIR and IC effectively treat LTrPs found in the gastrocnemius over acute and mid-term treatment protocols. Both groups had a significant effect on the number of LTrPs, ankle dorsiflexion ROM and the reduction of LTrP compression sensitivity. The statistical analyses identified MET PIR as the most effective method of reducing the presence of LTrPs and improving ankle dorsiflexion ROM than IC for both acute and mid-term treatment protocols. Therefore, this study concludes that MET PIR is the most effective form of treatment for LTrPs found in the gastrocnemius.
APPLICATIONS IN SPORT
Athletic therapists and sport related clinicians are recommended to use MET PIR in situations where LTrPs are found within the gastrocnemius. Clinicians should recognize that some athletes respond better or worse than the statements of this study and should apply the findings of this study case by case. However, MET PIR is a suitable treatment method to use in a variety of settings that an athletic therapist or clinician may be in, such as pre-game and post-game therapy, on-field therapy, and clinical therapy. Furthermore, MET PIR is suited to acute and mid-term treatment protocols for LTrP removal.
REFERENCES
- Brukner, P., Clarsen, B., Cook, J., Cools, A., Crossley, K., Hutchinson, M., McCrory, P., Bahr, R. and Khan, K. (2017) (a). Brukner and Khan’s clinical sports medicine, Vol 1. Sydney, Australlia: McGraw-Hill Education, 43.
- Celik, D., Mutulu, E.K. (2013). Clinical implication of latent myofascial trigger point. Current Pain and Headache Reports, 17 (8), 353-360.
- Chaitow, L. (2006) (a). Muscle Energy Techniques (2nd ed.). London, United Kingdom: Churchill Livingston, 139.
- Chaitow, L. (2006) (b). Muscle Energy Techniques (2nd ed.). London, United Kingdom: Churchill Livingston, 8-9.
- Dommerholt, J. (Ed.). (2011) (a). Myofascial trigger points: pathophysiology and evidence-informed diagnosis and management. London, United Kingdom: Jones and Barlett Publishers, 3.
- Dommerholt, J. (Ed.). (2011) (b). Myofascial trigger points: pathophysiology and evidence-informed diagnosis and management. London, United Kingdom: Jones and Barlett Publishers, 146-147.
- Dommerholt, J. (Ed.). (2011) (c). Myofascial trigger points: pathophysiology and evidence-informed diagnosis and management. London, United Kingdom: Jones and Barlett Publishers, 170.
- El Laithy, M.H. and Founda, K.Z. (2018). Effect of post isometric relaxation technique in the treatment of mechanical neck pain, Physical Therapy and Rehabilitation, 5(20), 1-6.
- Esperaza, D. Aladro-Gonzalvo, A.R. and Rybarczyk, Y. (2019). Effects of Local Ischemic Compression on Upper Limb Latent Myofascial Trigger Points: A Study of Subjective Pain and Linear Motor Performance, Hindawi Rehabilitation Research and Practice, 1-8.
- Finando, D. and Finando, S. (2005) (a). Trigger point therapy for myofascial pain, Vermont, Canada: Healing Arts Press, 17-18.
- Gilani, M.H., Obaid, S. and Tariq, M. (2018). Comparison between effectiveness of ischemic compression and muscle energy technique in upper trapezius myofascial trigger points. Isra Medical Journal, 10 (4), 230-234.
- Haritha, P., Shanthi, C. and Madhavi, K. (2015). Efficacy of post isometric relaxation versus static stretching in subjects with chronic nonspecific neck pain, International Journal of Physiotherapy, 2(6), 1097-1102.
- Han, S.C. and Harrison, P. (1997). Myofascial pain syndrome and trigger-point management, Regional Analgesia and Pain Medicine, 22 (1), 89-101.
- Islam, F., Arshad, K., Arif, M.A. and Bashir, M.S. (2017). Post isometric hamstring stretching; efficacy of post isometric hamstring stretching with and without cross frictional massage in football players, The Professional Medical Journal, 24(8), 1224-1231.
- Joshi, R. and Rathi, M. (2015). Effect of muscle energy technique versus positional release technique on pain and functions in patients with trapezitis- a comparative study, International Journal of Science and Research, 6(5), 2113-2115.
- Kumar, G.Y., Sneha, P. and Sivajyothi, N. (2015). Effectiveness of muscle energy technique, ischaemic compression and strain counterstrain on the upper trapezius trigger points: a comparative study.International Journal of Physical Education, Sports and Health, 1 (3), 22-26.
- Lewit, K. and Simons, D.G. (1984). Myofascial pain: relief by post-isometric relaxation. Archives of Physical Medicine and Rehabilitation, 65 (8), 452- 456.
- Lucas, K.R., Polus, B.I., and Rich, P.A. (2004). Latent myofascial trigger points: their effects on muscle activation and movement efficiency. Journal of Bodywork and Movement Therapies, 8, 160-166.
- Mahajan, R., Kataria, C. and Bansal, K. (2012). Comparative effectiveness of muscle energy technique and static stretching for treatment of subacute mechanical neck pain. International Journal of Health and Rehabilitation Science, 1 (1), 16-24.
- Mehdikhani, R. and Okhovatian, F. (2012). Immediate effect of muscle energy technique on latent trigger point of upper trapezius muscle, Clinical Chiropractic, 15, 112-120.
- Nambi, G.S., Sharma, R., Inbasekaran, D., Vaghesiya, A. and Bhatt, U. (2013). Difference in effect between ischemic compression and muscle energy technique on upper trapezius myofascial trigger points: comparative study, International Journal of Health and Allied Sciences, 2 (1), 17-22.
- Reed, M.L., Begalle, R.L. and Laudner, K.G. (2018). Acute effects of muscle energy technique and joint mobilisation on shoulder tightness in youth throwing athletes: a randomized controlled trial. The International Journal of Sports Physical Therapy, 13 (6), 1024-1031.
- Simons D.G., Travell, J.G. (1993). Myofascial pain and dysfunction: the trigger point manual, volume 2: the lower extremities. London, United Kingdom: Williams and Wilkins, 12.
- Simons, D.G., Travell, J.G. and Simons, L.S. (1999) (a). Myofascial pain and dysfunction: the trigger point manual volume 1: upper half of the body (2nd ed.). London, United Kingdom: Williams and Wilkins, 59-60.
- Simons, D.G., Travell, J.G. and Simons, L.S. (1999) (b). Myofascial pain and dysfunction: the trigger point manual volume 1: upper half of the body (2nd ed.). London, United Kingdom: Williams and Wilkins, 21-22.
- Thiyagarajan, S. (2012). A comparative study between the efficacy of post isometric relaxation versus post isometric relaxation with TENS on upper trapezius myofascial pain syndrome. Indian Journal of Physiotherapy and Occupational Therapy, 6(1), 196-199.
