Abstract
Much effort over the past 50 years has been devoted to research on training, but little is known about recovery after intense running efforts. Insufficient recovery impedes training and performance. Anecdotal evidence suggests that cold water immersion immediately following intense distance running efforts aids in next day performance perhaps by decreasing injury or increasing recovery. The purpose of this study was to compare 5 km racing performance after 24 hrs with and without cold water immersion. Twelve well-trained runners (9 males, 3 females) completed successive (within 24 hours) 5 km performance trials on two separate occasions. Immediately following the first baseline 5 km trial, runners were treated with ice water immersion for 12 minutes followed by 24 hrs of passive recovery (ICE). Another session involved two 5 km time trials: a baseline trial and another trial after 24 hrs of passive recovery (CON). Treatments occurred in a counterbalanced order and were separated by 6-7 days of normal training. ICE (20:08 ± 2.0 min) was not significantly different (p = 0.09) from baseline (19:59 ± 2.0 min). CON (19:59 ± 1.9 min) was significantly (p = 0.03) slower than baseline (19:49 ± 1.9 min). ICE heart rate (175.3 ± 7.6 b/min) was significantly (p = 0.02) less than baseline (178.3 ± 9.8 b/min), yet CON heart rate (177.3 ± 6.3 b/min) was the same as baseline (177.3 ± 7.3 b/min). ICE rate of perceived exertion (19.2 + 1.0) was significantly less (p = 0.03) than baseline (19.8 ± 0.5) while CON rate of perceived exertion (19.5 ± 0.8) was not significantly different (p = 0.39) from baseline (19.6 ± 0.8). Seven individuals responded negatively to ICE running a mean 24.0 ± 13.9 seconds slower than baseline. Nine individuals responded negatively to CON by running a mean 17.4 ± 12.1 seconds slower than baseline. Three individuals responded positively to ICE running a mean 20.33 ± 6.7 seconds faster during second day performance. Three individuals responded positively to CON by running a mean 13.3 ± 6.8 seconds faster than baseline. In general, cold water immersion minutely reduced the decline of next day performance, yet individual variability existed. Efficacy of longer durations of cold water immersion impact after 48 hrs and on distances greater than 5 km appear to be individual and need to be further explored.
Key words: cryotherapy, ice water immersion, passive recovery, running
Introduction
Recovery from hard running efforts plays a vital role in determining when a runner can run at an intense level again (Fitzgerald, 2007). Hard training, followed by adequate recovery, allows the body to adapt to the unusual stress and become better accustomed and more prepared for the same stress, should it occur again (Fitzgerald, 2007; Sinclair, Olgesby, & Piepenberg, 2003). Balancing hard efforts with periods of rest is essential in improving performance during endurance efforts.
The recovery process from endurance efforts tends to revolve around repairing damaged muscle fibers and replenishing glycogen stores (Gomez et al., 2002; Nicholas et al., 1997). Methods proposed to enhance recovery, such as cold water immersion, potentially decrease swelling and the severity of delayed onset of muscle soreness (DOMS), which possibly benefits endurance (i.e. running) and anaerobic performance (Higdon, 1998; Vaile, Gill, & Blazevich, 2007).
Cold water immersion is a common practice among collegiate and professional athletes following intense physical efforts. Anecdotal evidence from several National Athletic Trainers’ Association (NATA) collegiate head athletic trainers suggests that cooling the legs after a hard training effort may benefit the next day’s performance. Popular running and athletic magazines (e.g., Runner’s World, Running Times, etc.) have continually suggested that applying cold water to the legs of a runner facilitates a better perceived feeling for the next run on the following day. Yet, despite its widespread use there is no scientific data supporting the notion that cooling the legs after a hard distance running effort will improve performance 24 hrs later.
The use of cold as a treatment is as ancient as the practice of medicine, dating back to Hippocrates (Stamford, 1996). The therapeutic use of cold is the most commonly used modality in the acute management of musculoskeletal injuries. Running is a catabolic process, with eccentric muscle contractions leading to muscle damage. Applying cold to an injured site decreases pain sensation, improves the metabolic rate of tissue, and allows uninjured tissue to survive a post-injury period of ischemia, or perhaps allows the tissue to be protected from the damaging enzymatic reactions that may accompany injury (Arnheim and Prentice, 1999; Merrick, Jutte, & Smith, 2003). The use of cryotherapy, between sets of “pulley exercises” (similar to a seated pulley row), decreased the feelings of fatigue of the arm and shoulder muscles of 10 male weight lifters (Verducci, 2000), while other cryotherapy research involving recovery from intense anaerobic efforts has yielded equivocal results (Barnett, 2006; Cheung, Hume, & Maxwell, 2003; Crowe, O’Connor, & Rudd, 2007; Howatson, Gaze, & Van Someren, 2005; Howatson and Van Someren, 2003; Isabell et al., 1992; Paddon-Jones and Quigley, 1997; Sellwood et al., 2007; Vaile, Gill, & Blazevich, 2007; Vaile et al., 2008; Yackzan, Adams, and Francis, 1984). However, methods of cryotherapy effective for enhancing recovery from distance running efforts have not been examined.
Long duration or high intensity running contributes to muscle cell damage (Fitzgerald, 2007; Noakes, 2003). Edema, a by-product of muscle damage can cause reduced range of joint motion. Because cryotherapy has been shown to decrease inflammation (Dolan et al., 1997; O’Conner and Wilder, 2001), it is logical to assume that this treatment may reduce the severity of DOMS. Less pain may permit an athlete to push themselves harder potentially improving performance. Despite the fact that previous research has shown that 24 hrs alone is not sufficient recovery from 5 km running performance (Bosak, Bishop, & Green, 2008), it might be possible that combining cold water immersion with 24 hrs of recovery could potentially hasten the recovery process. Therefore, the purpose of this study was to compare 5 km racing performance after 24 hrs of passive recovery with and without cold water immersion.
Methods
Participants:
Participants for the study were 12 well trained male (n = 9) and female (n = 3) runners currently engaged in rigorous training. Runners from the local road running and track club, local triathlon competitors, as well as former competitive high school and college runners, were recruited by word of mouth. Participant inclusion criteria included the following: 1) Subjects must have been currently involved in a distance running training program; 2) Their 5 km times previously run had to be at least 16-22 min for male runners or 18-24 min for female runners; 3) They had to be currently averaging at least 20-30 miles (running) per week; 4) They had to have previously completed at least five 5 km road or track races; 5) They had to have a VO2max of at least 45 ml/kg/min (females) or 55 ml/kg/min (males); and 6) They had to provide sufficient data (from running history questionnaires, physical activity readiness questionnaires, and health readiness questionnaires) that reflected good health.
Participants completed a short questionnaire regarding their running background, racing history, and current training mileage. All participants were volunteers and signed a written informed consent outlining requirements as well as potential risks and benefits resulting from participating.
Procedures:
Participants were assessed for age, height, body weight, and body fat percentage using a 3-site skinfold technique (Brozek and Hanschel, 1961; Pollock, Schmidt, & Jackson, 1980). Participants were fitted with a Polar heart rate monitor, and then completed a graded exercise test (GXT) to exhaustion lasting approximately 12-18 min. VO2max, heart rate (HR), and ratings of perceived exertion (RPE) were collected every minute.
All GXTs were completed on a Quinton 640 motorized treadmill. The test began with a 2 min warm-up at 2.5 mph. Speed was increased to 5 mph for 2 min, followed by 2 min at 6 mph, 2 min at 7 mph, and 2 min at 7.5 mph. At this point, incline was increased two percent every 2 min thereafter until the participant reached volitional exhaustion (i.e. they felt like they could no longer continue running at the required speed and grade). Once the participant reached volitional exhaustion, they were instructed to cool down until they felt recovered.
Approximately five days later, participants performed their first 5 km race (performance trial) between the hours of 6:30 am to 7:30 am. The time of day for each performance trial was consistent throughout the entire study. All performance trials were completed on a flat hard-surfaced 0.73 mile loop. Prior to each trial, participants completed visual analog scales, before and after a 1.5 mile warm-up run, regarding their feelings of fatigue and soreness within local muscle groups (quadriceps, hamstrings, gastrocnemius), and for lower and total body muscle groups. Visual analog scales were 15 cm lines, where participants placed an “X” on the line indicating their feelings (with 0 = no fatigue or soreness and 15 = extreme fatigue or soreness). The focus of the visual analog scales was to determine if participants felt the same before the start of every time trial. Participants were also required to rate their perceived exertion (RPE) after the warm-up and prior to the start of each 5 km, during each trial, and at the end of each performance trial to determine if feelings of effort remained consistent between each trial, as well as during each lap and at the end of each trial.
Runners underwent a 1.5 mile warm-up prior to every 5 km performance trial (Kaufmann and Ware, 1977). Participants completed four 5 km performance trials within nine days. Two 5 km performance trials (baseline and CON) were separated by 24 hrs of passive recovery. Passive recovery was deemed as no exercise or extensive physical activity during the allotted recovery hours. Two 5 km performance trials (baseline and ICE) were also separated by 24 hrs of passive recovery, but with 12 minutes of 15.5ºC water immersion immediately following the baseline trial. The two sessions of 5 km performance trials were counterbalanced and were separated by 6-7 days of normal training. Each trial session therefore, had a separate baseline preceded by 24 hrs of passive recovery.
Ideal cryotherapeutic water temperature has not been determined, yet various head collegiate athletic trainers prefer that the water temperature does not dip below 13ºC (55.5ºF) since many people find water temperatures below 13ºC uncomfortable (O’Connor and Wilder, 2001). Also, the duration of ice baths generally lasts 10-15 minutes and is usually applied immediately after a hard training session (Crowe, O’Connor, & Rudd, 2007; Schniepp et al., 2002; Vaile et al., 2008). Hence, in this study, 15.5ºC (60ºF) was the temperature for the cold water and the athletes were immersed for 12 min.
During each time trial, average heart rate and ending RPE were recorded in order to determine if effort for each 5 km was consistent. All participants competed with runners of similar ability to simulate race day and hard training conditions, while verbal encouragement was provided often and equally to each participant. At the end of every performance trial, each runner was instructed to complete a low intensity 1.5 mile cool-down. Each total testing trial required approximately 60 min.
Statistical Analysis:
Basic descriptive statistics were computed. Repeated measures of analysis of variance (ANOVA) were employed for making comparisons between CON and baseline and PAS and baseline performance trials for the following variables: finishing times, HR, RPE, and fatigue or soreness responses. All statistical comparisons were made at an a priori p < .05 level of significance. Data were expressed as group mean + standard deviation and individual results.
In order to evaluate individual responses, data from each participant’s first run was compared to the second run using a paired T-test. The least significance group mean difference (p < 0.05) was determined and group mean finishing time was adjusted to determine the amount of change in seconds needed for significance to occur. The time change between the first trial run and the adjusted trial run baseline was divided by the first trial run and expressed as mean number of seconds or percent for both the ICE (9.3 seconds or 0.8%) and CON (9.5 seconds or 0.8%) trials. The percent values were applied to each individual baseline time in order to determine how many seconds (positive or negative) the second performance trial time had to be over or under the first performance trial, in both CON and ICE conditions, to quantify as a response. Participants were then labeled as non-responders, positive-responders (faster after treatment), and negative-responders (slower after treatment).
Results
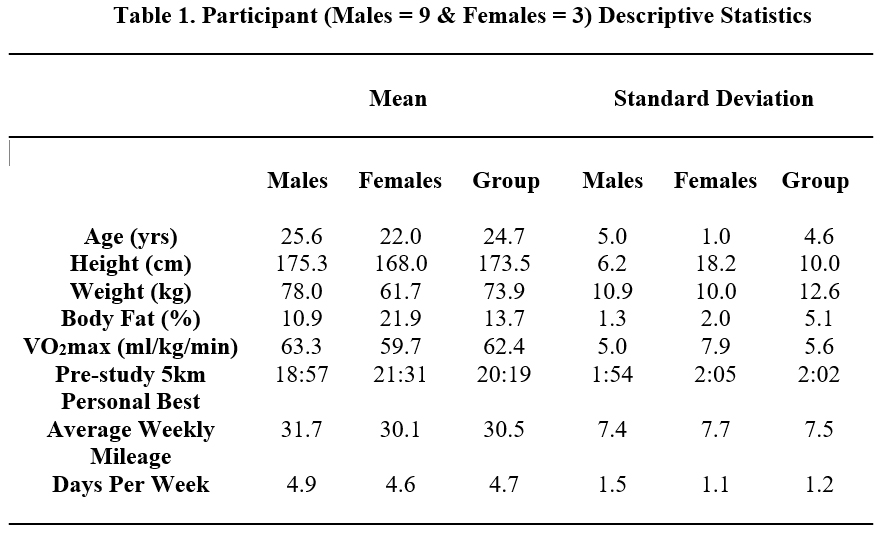
Descriptive characteristics are found in Table 1. The participants were between the ages of 18 and 35 (the majority of subjects were between ages 20-28) years. All participants were trained runners or triathletes (where running was their specialty event).
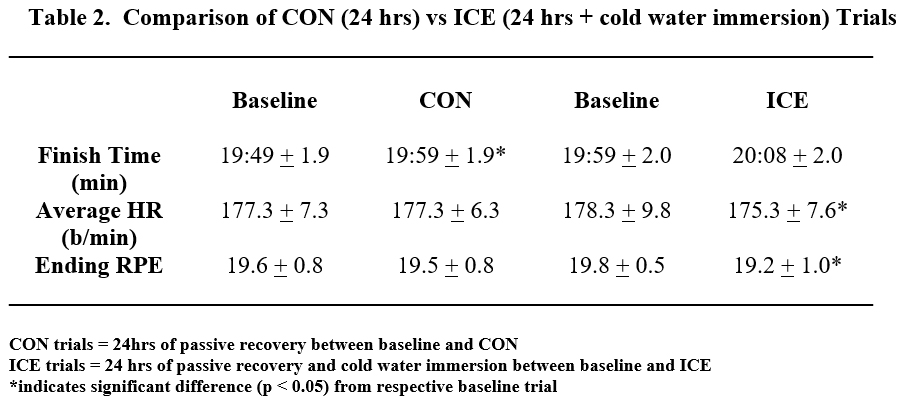
Mean finishing times, HR, and RPE for CON and ICE trials are found in Table 2. CON was significantly (p = 0.03) slower (10 seconds) than baseline, where as ICE was not significantly different (p = 0.09) from baseline. No significant differences were found between CON HR vs. baseline, but ICE HR was significantly (p = 0.01) less than baseline. No significant differences (p = 0.39) were found between CON RPE and baseline, yet ICE RPE was significantly (p = 0.03) less than baseline.
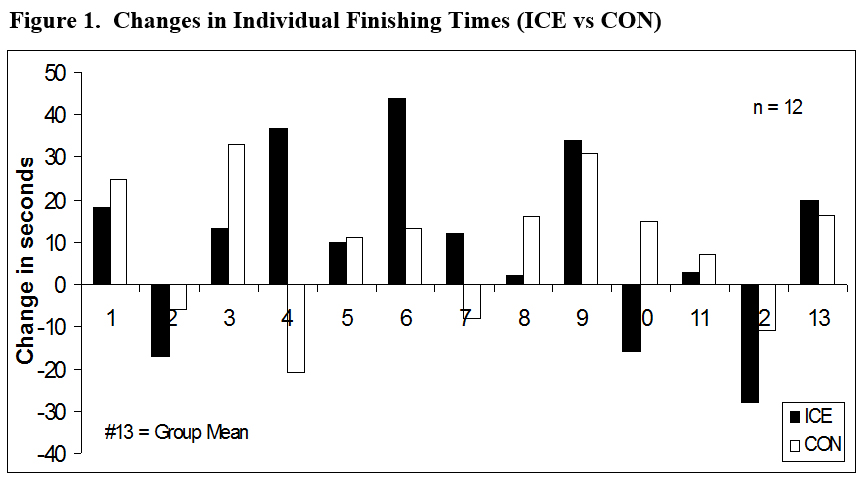
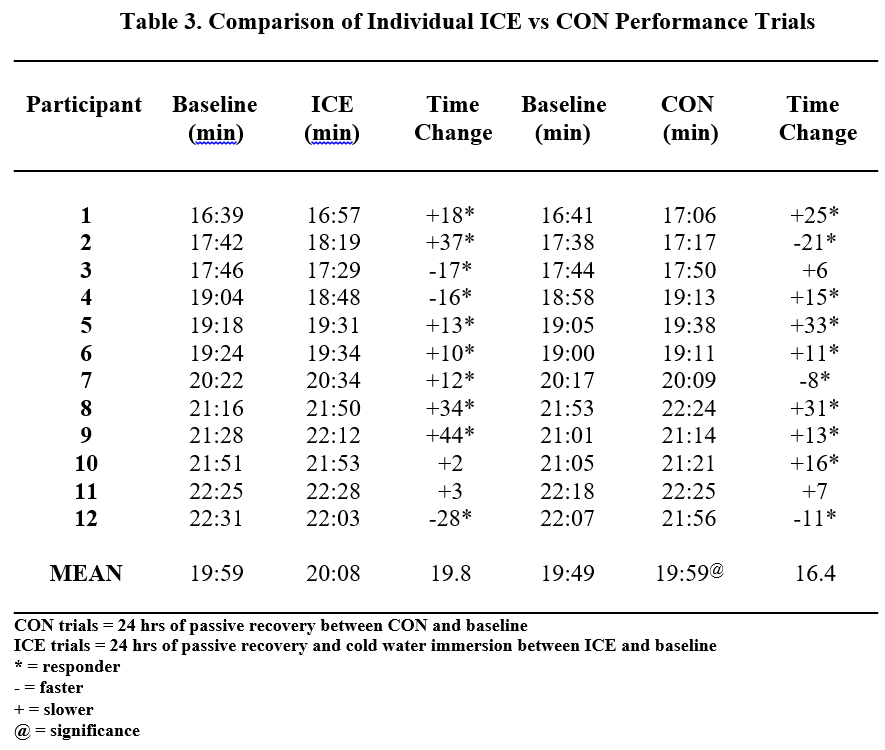
Figure 1 shows individual changes in finishing times for all CON and ICE performance trials. To be considered a non-responder, the individual time change had to fall within 0.8% of baseline performance for ICE and CON. Positive and negative responders (Table 3) were identified when individual time change was greater than 0.8% for CON and ICE trials, with a positive responder being one whose second performance trial time improved (expressed as a negative value) and a negative responder being one whose second performance trial time slowed (expressed as a positive value).
Seven individuals responded negatively to ICE by running a mean 24.0 ± 13.9 seconds slower during the second trial (Table 3). Three individuals responded positively to ICE by running a mean 20.3 ± 6.7 seconds faster than baseline. Two individuals were considered non-responders to ICE with a mean time change of 2.5 ± 0.7secs.
Seven individuals responded negatively to CON by running a mean 20.6 ± 9.0 seconds slower than baseline (Table 3). Three individuals responded positively to CON by running a mean 13.3 ± 6.8 seconds faster than baseline. Two individuals were non-responders to the CON trials with a mean time change of 6.5 ± 0.7 seconds. It is important to note that the seven individuals who were negative responders to ICE were not the same seven participants who responded negatively to CON. Also, the three participants who responded positively to ICE were not the same three individuals who responded positively to CON. Finally, the non-responders to ICE were not the same non-responders to CON.
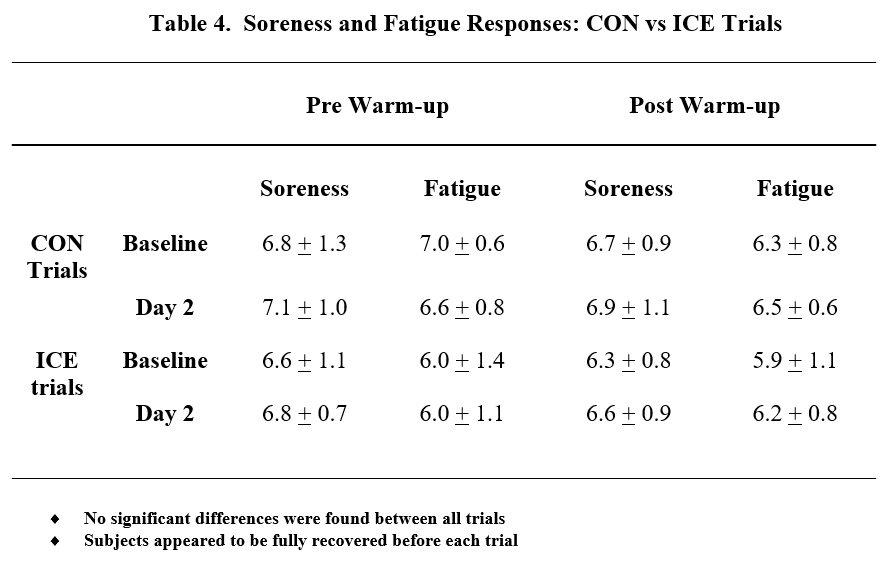
Soreness and fatigue scores (Table 4) on the pre-and post-warm-up fatigue or soreness visual analog scales were not significantly different between CON and baseline versus ICE and baseline.
Discussion
The effects of cold-water immersion on recovery and next day performance in 5 km racing have not been previously evaluated. Therefore, the primary purpose of this study was to compare 5 km running performance after 24 hrs of passive recovery with and without cold water immersion. This study appeared to indicate that cold water immersion does not dramatically help performance (regarding the group of runners as a whole) during second day 5 km trials.
Twenty-four hours of passive recovery may allow for normalization of muscle and liver glycogen, yet muscle function and performance measures may not be fully recovered (Foss and Keteyian, 1998). Hence, 24 hrs of recovery, by itself, may not be sufficient to allow for a return to optimal performance (Bosak, Bishop, & Green, 2008). When racing (e.g., a 5 km distance) on consecutive days, race times may be slower on the second day due to magnified perception of pain and impaired muscle function associated with DOMS (Brown and Henderson, 2002; Fitzgerald, 2007; Galloway, 1984). Since cold water immersion may speed up the recovery process (Arnheim and Prentice, 1999; Vaile et al., 2008) it is logical to assume that cold water immersion immediately after a 5 km race or workout could attenuate soreness potentially minimizing performance decrements on successive days.
There were no significant (p = 0.09) differences in 5 km performance between ICE and baseline, indicating that mean performance during ICE was not significantly slower (9 seconds) than baseline (refer to Table 2). However, CON performance was significantly (p = 0.03) slower (10 seconds) than baseline. Hence, due to significant differences occurring between ICE and baseline, it appears that cold water immersion slightly attenuated the rate of decline on successive 5 km time trial performance. However, the time difference between CON and baseline versus ICE and baseline was a mere second. Therefore, from a practical standpoint, cold water immersion was no more beneficial than CON on successive 5 km performance.
Despite the minimal differences between CON (10 seconds) and ICE (9 seconds) trials regarding mean time change, it is important to focus on the effects of cold water immersion on individual runners (Figure 1). Because some runners ran slower during successive performance trials while other runners ran faster, the mean finishing times do not necessarily give a true impression of the benefits or liabilities of the specific treatments involved in this study. As it is with most ergogenic aids, individual variability suggests what works (e.g., ice) for one person may not work the same for another person. It is possible that the treatment may often not have an effect at all, as similar to what occurred with several prior anaerobic performance studies (Barnett, 2006; Cheung, Hume, & Maxwell, 2003; Crowe, O’Connor, & Rudd, 2007; Howatson, Gaze, & Van Someren, 2005; Howatson and Van Someren, 2003; Isabell et al., 1992; Paddon-Jones and Quigley, 1997; Sellwood et al., 2007; Vaile et al., 2008), which was also the case in this study as two individuals were considered non-responders to ICE with a mean time change of 2.5 ± 0.7 seconds between ICE and baseline, while two other participants were non-responders to CON with a mean time change of 6.5 ± 0.7 seconds between CON and baseline.
Three individuals responded positively (Table 3) to ICE, running a mean 20.33 ± 6.7 seconds faster, indicating that cold water immersion may have actually allowed these individuals to run faster on the second day. However, 3 different individuals responded positively to CON, running a mean 13.3 ± 6.8 seconds faster than baseline. The mechanism by which cold water immersion aids in recovery, from endurance performance, remains somewhat unclear and equivocal (Schniepp et al., 2002; Vaile et al., 2008). Yet, several runners who did run faster during ICE trial, verbally indicated that prior to the second trial, their legs felt better (regarding fatigue and soreness) than they had prior to CON. Thus, the notion of feeling better may have allowed the runners to perform faster.
Seven individuals responded negatively (Table 3) to ICE, running a mean 24.0 ± 13.9 seconds slower. However, they were not the same seven individuals who responded negatively to CON, who ran an average of 20.6 ± 9.0 seconds slower than baseline. As was the case with Schniepp et al. (2002) endurance cycling recovery study and various anaerobic performance studies (Crowe, O’Connor, & Rudd, 2007; Sellwood et al., 2002; Vaile et al., 2008; Yackzan, Adams, & Francis, 1984), it appears ICE may have had a more negative effect, for these individuals, on second day performance compared to CON.
Three individuals responded positively to CON running a mean 13.3 ± 6.8 seconds faster during the second day performance trial. It is unclear why some participants ran faster during CON. There were no consistent patterns of HR and increased or decreased performance with all participants during all CON and ICE trials. As a group, no significant differences were found between CON vs. baseline, regarding HR (p = 1.00) and RPE (p = 0.39), despite significant differences (p = 0.04) occurring in mean finishing time. However, mean finishing times for ICE were similar, yet significant differences were found between ICE vs. baseline for both HR (p = 0.01) and RPE (p = 0.03). Hence, there does not appear to be a consistent pattern between performance times and HR and/or RPE.
It can be assumed that a lower HR may be associated with slower times, since HR and intensity levels tend to be linearly related. However, only participants 1, 5, and 6 consistently ran slower during both CON and ICE second day performances with lower HR during both trials. During the ICE trials, only participants 1, 5, 6, and 9 ran slower and had a lower HR. During the CON trials, only 1, 3, 5, 6, ran slower and had a lower HR. Also, soreness and fatigue scores (Table 4) on the pre and post warm-up fatigue or soreness visual analog scales were not significantly different between CON and baseline versus ICE and baseline. These results indicate that all runners tended to feel the same prior to each second day 5 km trial. Therefore, since inconsistencies exist between HR and performance trials and no significant differences were found regarding RPE and fatigue or soreness visual analog scales, it is assumed that each participant completed each trial with similar effort.
Conclusion
The current findings of this study suggest that cold water immersion does not sufficiently enhance recovery (specifically regarding the group of runners as a whole). However, three runners benefited from cold water immersion. Hence, what works for one person may not work for another person. Thus, it may be beneficial for runners to undergo this protocol in order to see which type of recovery method improves their recovery process. Secondly, the results of the study may give credence to some runners’ perception of feeling better due to cold water immersion after a hard running effort. However, one should remember that individual variability existed in response to treatment (ice immersion) within the current study. Future research is needed to see if a greater length of time or slightly lower water temperature in cold water immersion will decrease the rate of decline more or if the effects of cold water immersion are even more predominant on second day performance of distances greater than 5 km.
References
Arnheim, D. D., & Prentice, W. E. (1999). Essentials of athletic training (4th ed.). Boston, MA: McGraw-Hill.
Barnett, A. (2006). Using recovery modalities between training sessions in elite athletes: Does it help? Sports Medicine, 36 (9), 781-796.
Bosak, A., Bishop, P., & Green, M. (2008). Comparison of 5km racing performance after 24 and 72 hours of passive recovery. International Journal of Coaching Science (In Review).
Brown, R. L., & Henderson, J. (2002). Fitness Running (2nd ed.). Champaign, IL: Human Kinetics.
Brozek, J., & Hanschel, A. (1961). Techniques for measuring body composition. Washington, DC: National Academy of Sciences.
Cheung, K., Hume, P., & Maxwell, L. (2003). Delayed onset muscle soreness: treatment strategies and performance factors. Sports Medicine, 33 (2), 145-164.
Crowe, M. J., O’Connor, D., & Rudd, D. (2007). Cold water recovery reduces anaerobic performance. International Journal of Sports Medicine, 28 (12), 994-998.
Dolan, M. G., Thorton, R. M., Fish, D. R., & Mendel, F. C. (1997). Effects of cold water immersion on edema formation after blunt injury to the hind limbs of rats. The Journal of Athletic Training, 32, 233-238.
Fitzgerald, M. (2007). Brain Training for Runners. New York, NY: Penguin Group.
Foss, M. L., & Keteyian, S. J. (1998). Fox’s Physiological Basis for Exercise and Sport. Ann Arbor, MI: McGraw-Hill.
Galloway, J. (1984). Galloway’s Book on Running. Bolinas, CA: Shelter Publications.
Gomez, A. L., Radzwich, R. J., Denegar, C. R., Volek, J. S., Rubin, M. R., Bush, J.A., Doan, B.K., et.al. (2002). The effects of a 10-kilometer run on muscle strength and power. Journal of Strength and Conditioning Research, 16, 184-191.
Higdon, H. (1998). Smart Running. Emmaus, PA: Rodale Press Inc.
Howatson, G., Gaze, D., & Van Someren, K. A. (2005). The efficacy of ice massage in the treatment of exercise-induced muscle damage. The Scandinavian Journal of Medicine and Science in Sports, 2005, 15 (6), 416-422.
Howatson, G. & Van Someren, K. A. (2003). Ice massage: Effects on exercise-induced muscle damage. The Journal of Sports Medicine and Physical Fitness, 43 (4), 500-505.
Isabell, W. K., Durrant, E., Myrer, W., & Anderson, S. (1992). The effects of ice massage, ice massage with exercise, and exercise on the prevention and treatment of Delayed Onset Muscle Soreness. The Journal of Athletic Training, 27 (3), 208-217.
Kaufmann, D. A. & Ware, W. B. (1977). Effect of warm-up and recovery techniques on repeated running endurance. The Research Quarterly, 2, 328-332.
Merrick, M. A., Jutte, L. S., & Smith, M. E. (2003). Cold modalities with different thermodynamic properties produce different surface and intramuscular temperatures. Journal of Athletic Training, 38, 28-35.
Nicholas, C. W., Green, P. A., Hawkins, R. D., & Williams, C. (1997). Carbohydrate intake and recovery of intermittent running capacity. International Journal of Sport Nutrition, 7, 251-260.
Noakes, T. (2003). Lore of Running (4th ed.). Champaign, IL: Human Kinetics.
O’Conner, F. G., & Wilder, R. P. (2001). Textbook of Running Medicine. New York, NY: McGraw-Hill.
Paddon-Jones, D. J., & Quigley, B. M. (1997). Effects of cryotherapy on muscle soreness and strength following eccentric exercise. The International Journal of Sports Medicine, 18 (8), 588-593.
Pollock, M. L., Schmidt, D. H., & Jackson, A. S. (1980). Measurement of cardiorespiratory fitness and body composition in the clinical setting. Comprehensive Therapy, 6, 12-27.
Schniepp, J., Campbell, T. S., Powell, K. L., & Pincivero, D. M. (2002). The effects of cold water immersion on power output and heart rate in elite cyclists. Journal of Strength and Conditioning Research, 16 (4), 561-566.
Sellwood, K. L., Bruker, P., Williams, D., Nicol, A., & Hinman, R. (2007). Ice-water immersion and delayed-onset muscle soreness: a randomized controlled trial. British Journal of Sports Medicine, 41 (6), 392-397.
Sinclair, J., Olgesby, K., & Piepenburg, C. (2003). Training to Achieve Peak Running Performance. Boulder, CO: Road Runner Sports Inc.
Stamford, B., Giving injuries the cold treatment. (1996). The Physician and Sports Medicine, 23, 1-4.
Vaile, J., Gill, N. D., & Blazevich, A. J. (2007). The effect of contrast water therapy on symptoms of delayed onset of muscle soreness. Journal of Strength and Conditioning Research, 21 (3), 697-702.
Vaile, J., Halson, S., Gill, N., & Dawson, B. (2008). Effect of hydrotherapy on recovery from fatigue. International Journal of Sports Medicine, 29 (7), 5:39-544.
Vaile, J., Halson, S., Gill, N., & Dawson, B. (2008). Effect of hydrotherapy on the signs and symptoms of delayed onset muscle soreness. European Journal of Applied Physiology, 102(4), 447-455.
Verducci, F. M. (2000). Interval cryotherapy decreases fatigue during repeated weight lifting. The Journal of Athletic Training, 35, 422-426.
Yackzan, L., Adams, C., & Francis, K. T. (1984). The effects of ice massage on delayed muscle soreness. The American Journal of Sports Medicine, 12 (2), 159-165.
Appendices