Throughout the centuries, dietary intake has been a source of concern to athletes in search of an ergogenic edge over opponents.
It wasn’t until 1866 that it was demonstrated that there was insignificant, if any use of protein as a fuel during exercise. Since that time, innumerable studies have refuted the notion that a high protein intake will enhance athletic performance.
Since the conclusion of the Kraus-Weber Tests in the 1950s, there has been ever- increasing awareness and concern for cardiopulmonary fitness and health in Americans. Endurance type activities such as Nordic skiing, cycling, running, triathalons, and swimming have become in vogue, and as a result, more intense attention has been devoted to dietary manipulations which may provide an ergogenic effect, thus prolonging time to exhaustion, or delaying the onset of blood lactate accumulation (OBLA) in an attempt to compete at a higher intensity, longer.
The classic study by Christensen and Hansen in 1939 established the effect of a high carbohydrate diet upon endurance time, and that pre-exercise glycogen levels exerted an influence in time to exhaustion. Subsequently, it was discovered that if an athlete, after depleting glycogen reserves, consumed a high carbohydrate diet for two to three days prior to an athletic event, there would in fact be higher glycogen levels than prior to exercise. This “supercompensation” effect became the basis for carbohydrate loading undertaken by endurance athletes.
Therefore, the concentration of muscle and liver glycogen prior to exercise plays an important role in endurance exercise capacity. In exhaustive exercise many studies have observed significant depletion of both liver and muscle glycogen. It is interesting to recognize that the point of exhaustion seems to occur upon the depletion of liver glycogen. Conversely, muscle glycogen reserves, though significantly lower are only 65-85% depleted, versus the 85-95% depletion exhibited for liver glycogen. This should make it readily apparent that liver glycogen is an integral determining factor in an athlete’s time to exhaustion. It follows that endurance athletes who maintain a daily regimen of endurance training without glycogen repletion may severely deplete their glycogen reserves.
Glycogen, the major reservoir of carbohydrate in the body, is comprised of long chain polymers of glucose molecules. The body stores approximately 450-550 grams of glycogen within the muscle and liver for use during exercise. At higher exercise intensities, glycogen becomes the main fuel utilized. Depletion of liver glycogen has the consequence of diminishing liver glucose output, and blood glucose concentrations accordingly. Because glucose is the fundamental energy source for the nervous system, a substantial decline in blood glucose results in volitional exhaustion, due to glucose deficiency to the brain. It appears that the evidence presented in the literature universally supports the concept that the greater the depletion of skeletal muscle glycogen, then the stronger the stimulus to replenish stores upon the cessation of exercise, provided adequate carbohydrate is supplied.
Though most of the evidence presented on glycogen is related to prolonged aerobic exercise, there is evidence that exercise mode may play a role in glycogen replenishment, with eccentric exercise exhibiting significantly longer recovery periods, up to four days post-exercise. Muscle fiber type is another factor implicated in the replenishment of glycogen in athletes, due to the enzymatic capacity of the muscle fiber, with red fiber appearing to be subjected to a greater depletion, but also undergoing repletion at a significantly grater rate.
Though early literature appeared to indicate that the time course of glycogen replenishment after exercise-induced depletion was 48 hours or more, more recent data have controverted this thought. One study reported that a carbohydrate intake totaling up to 550-625 grams per day was found to restore muscle glycogen stores to pre-exercise levels within the 22 hours between exercise sessions. The findings of this study were supported by second study in which a carbohydrate intake of 3100 kcal resulted in complete resynthesis of glycogen within 24 hours.
There also appears to be a two-hour optimal window immediately after the cessation of exercise for the administration of carbohydrates. Simple carbohydrates appear to be the preferred replacement during this replenishment period.
Normally, 2% of glycogen is resynthesized per hour after the initial 2 hours immediately after exercise. With administration of 50 grams of carbohydrate every 2 hours, the rate rose to 5% per hour, but did not rise when additional carbohydrate was administered. Administration of .7grams per kg body weight every two hours is another strategy that appears to maximize the rate of glycogen resynthesis. There is also some evidence that even smaller loads (28 grams every 15 minutes) may induce even greater repletion rates.
Therefore, at least 20 hours are required to recover muscle glycogen stores, even when the diet is optimal. So, athletes working out two times per day should complete one workout at a diminished workload to relieve the reliance on glycogen reserves.
The principle of glycogen resynthesis and supercompensation has great practical implications, not only in athletics, but also within industry for workers who consistently undergo depletion of glycogen stores due to prolonged bouts of exertion, or extended lifting tasks which would be glycolytic in nature; due to the duration, and also the myofibrillar ischemia induced by static contractions.
Submitted by: R.T. Couture, J. Tihanyi and M. St-Aubin
ABSTRACT
Changes in cognitive strategies can improve performances and lessen perceived fatigue during distance activities (Padget & Hill, 1989). However, such changes may be difficult and annoying for participants (Masters & Lambert, 1989). This study identified subjects’ preferred cognitive strategies and examined the effects of a complementary cognitive strategy. Twenty-five subjects performed an 800 meter free-style swim while being timed and assessed for heart rate. One week later, subjects read a Behavioral Instruction Sheet (BIS), appropriate for their style in the first swim and followed it during the second swim. Results showed that associative thinking was used more frequently than dissociative thinking by 73%, t(21) = 6.68, p<.05. No significant differences were found from the first to the second swim in performance times, RPE and heart rates with the exception of more muscular fatigue in the second swim t (16) = -2.17, p<.05. This study suggests that cognitive strategy training can not be completely associative or dissociative.
INTRODUCTION
Various forms of cognitive self-control strategies have long been used for optimizing endurance performance. In some instances, individuals use distracting forms of thinking to endure longer sustained performance perceive less fatigue and perform faster than those strategies focusing on the task (Gill & Strom, 1985; Padget & Hill, 1989;). Yet these results are not without controversial findings (Masters & Lambert, 1989; Schomer, 1987). World-class marathoners tend to apply focusing techniques almost invariably during marathon races to maintain an accurate awareness of their bodily function, tension, pain and discomfort (Morgan, 1978). However, when training, runners tend to prefer a dissociative strategy (Pennebaker & Lightner, 1980).
A developing body of research supports the notion that some distance runners can mentally separate themselves from the inherent pain and fatigue resulting from marathon running. Morgan and Pollock (1977) suggest that two cognitive strategies are frequently used by runners; “association” and “dissociation”. They theorize that dissociation is more pleasurable as it enables individuals to reduce “anxiety, effort sense and general discomfort” (Morgan, 1978, p. 46). It is also thought that dissociation strategies allow marathon runners to persevere through temporary zones of boredom (Schomer, 1986). However, Morgan and Pollock (1977) found that world-class marathoners tend to apply associative techniques almost invariably during marathon races to maintain an accurate awareness of their bodily function, tension, pain and discomfort (Morgan, 1978). Morgan and Pollock (1977) describe runners’ associative strategies as: scanning their body to identify painful or tense areas and thus remember to lessen muscle tension while implementing feelings of relaxation; and thinking of their pace and race strategy (Morgan, 1978).
Rushall and Shewchuk (1989) examined the effects of thought content instructions on swimming performance. Using three types of thought instructions on training performances, swimmers completed two 400-meter effort swims and one set of 8 x 100- meter swims. Such types of strategies like positive thinking and mood word conditions made all swimmers improve their workout performance in at least two of the three conditions during the 100-meter repeat task. Such findings in thought manipulations are encouraging yet Weinberg, Smith, Jackson and Gould (1984) suggest that some athletes find it difficult to change their cognitive strategies (from dissociative thoughts to associative thinking or vice versa). In fact, some subjects find it bothersome and annoying to change their existing cognitive strategies (Masters & Lambert, 1989; Weinberg, Smith, Jackson & Gould, 1984).
While some studies have examined the effects of both cognitive strategies, few if any studies have ever considered identifying the subjects’ preferred choice of cognitive strategy and complementing their current predominant strategy. The purpose of this study was two-fold: to identify subjects’ preferred cognitive strategies during distance swimming and to examine the effects of using a cognitive strategy that is complimentary to the one being used by swimmers.
METHODOLOGY Subjects
A total of 22 subjects (11 males and 11 females) from a University Masters Swim Club volunteered to swim two 800 meter free-style swims, one week apart. Subjects varied in age from 19 to 45 years old (m=27) and normally swam between 500 m and 12,500 m per week (m= 4,490 metres).
Measurements
Pre-Swim Questionnaire
The pre-swim questionnaire consisted of gathering general and demographic information (i.e., why do they swim distances? preferred cognitive thought patterns when swimming, etc.).
Timed Performance
Swimmers’ performances were timed during both swims with stopwatches, accurate to 1/100th of a second. Timers were briefed on the proper procedures and were familiarized with the stopwatches prior to the study. Subjects were told that this was not a race and that they should swim their normal speed.
Heart Rate
Before swimming, the subjects were fitted with a Vantage XL Sport Tester transmitter and receiver that recorded time and heart rate every 15 seconds from the moment they started the swim to the end. This modality has been used extensively to train and measure athletes (Daniels & Landers, 1981). The data was then down-loaded via an interface unit to a computer for processing.
Subjective Appraisal of Cognitive Thoughts
(SACT; Schomer, 1986) The SACT consists of 10 categories, in which each descriptor relates to a specific cognitive attentional style (associative or dissociative). Subjects were asked to circle all those descriptors that came to mind while swimming. Depending on the number of associative or dissociative descriptors the subject was identified as preferring a particular style of cognitive thinking. Schomer (1986) established the reliability and validity of the statements by examining 109 recordings taken from marathoners, four times per month. After transcribing runners’ personal conversations, Schomer inspected the scripts for “recurrent thoughts on task-related and task-unrelated material”. Categories were proposed and rationalized based on a “pronounced attentional focus”. The reliability and validity of 10 sub-classifications emerged (Schomer, 1986).
A pilot study with 20 swimmers was conducted by the present investigators to examine the construct validity of the categories as outlined by Schomer. For the swimmers, it indicated that comprehension of the sub-classification titles was poor. Consequently, the titles were re-worded in a general context while using the same content and examples employed by Schomer (1986) in his description of the subcategories.
Perceived Fatigue Questionnaire
(PFQ; Pennebaker and Lightner, 1980) The PFQ measures changes in perceived fatigue. It contains 10 physiological symptoms related to fatigue (dizziness, sore eyes, headache, etc.) which are measured on a scale from 1 to 100. For each symptom, subjects mark with a slash how they feel (e.g., 0 = not at all dizzy to 100 = the worst feeling of dizziness ever). All scores are summed to provide a total symptom index of fatigue. The scalar properties of these symptoms are found in Pennebaker & Skelton (1978).
Rate of Perceived Exertion
(RPE; Borg, 1982) The RPE scale is a 15-point instrument ranging from 6 to 20. The instrument has several identifiers at every uneven number (e.g., 7 “very very light” and 19 “very very heavy”). It has been found to correlate linearly with heart rate. Because of its positive relationship with heart rate, the RPE scale was an appropriate measurement for this study. In the present study, the RPE was printed on a large cardboard and shown to the swimmers after each swim.
Post-Swim Questionnaire
Following the second swim, swimmers in the associative and dissociative groups were asked to evaluate the effectiveness of the strategies. This questionnaire identified the extent to which the assigned strategy was used during the swim.
Procedure
After signing a consent form and being informed of the results’ confidentiality, the subjects prepared for the swim. Prior to entering into the pool, subjects answered a short Pre-Swim Questionnaire. Subjects were cautioned that this was not a race. All swimmers wore a waterproof wrist-mounted heart rate receiver and a transmitter around the chest. A total of eight swimmers (one swimmer per lane) swam at any one time. Staggered starts (one minute apart) were used to lessen the “motivation” variable of competition against peers. This enabled the swimmers to use dissociative strategies if they so wished in the first swim. All swimmers stopped at the end of 800 meters when they saw a red flutter board being waved underwater as they approached the end of the pool. This procedure was chosen to minimize potential disruptions with swimmers who were not finished their swim. Swimmers’ times were taken by trained individuals who were supervised by the researchers.
RESULTS
Subjects in this study generally commented that they swam for fitness (65.6%) and relaxation (19.4%). The pre-swim questionnaire revealed the swimmer’s preference for a certain type of strategy; either associative (78.1%), dissociative (9.6%) or a mixture of both (12.3%). Following the swim, results showed that swimmers preferred association thinking by 73%, a significant difference t(21)=6.68, p<.05 from dissociative thinking. Associative thinking was found to occur significantly more in the middle of the swim than near the end F(2,24)=3.87; p<.035.
Table 1: Impressions of the Behavioral Instruction Sheet According to Their Cognitive Strategy
DESCRIPTORS
During the Swim
Easy to Use
Helpful
Effective
Less Boredom
Less Pain
First part of the swim
80
60
60
40
0
Middle part of the swim
60
80
80
40
80
Latter part of the swim
40
80
80
60
80
Note. Scores are based on a 100 point scale.
Though a number of descriptors were offered in the Perceived Fatigue Questionnaire, subjects generally commented of more muscular fatigue in the second swim t (16) = -2.17, p<.05. No statistical changes were found in subjects’ swimming time, RPE and heart rates from the first to the second swim.
Subjects rated the BIS to be easy to use (m=71), helpful (m=69) and effective (m=63), on a 100 point scale. Boredom (m=60) and pain (m=51) were also reduced.
Subjective Appraisal of their Cognitive Strategy during the Second Swim
Generally, 57% of subjects found the second swim easier (86% associative and 14% dissociative). The associative thinkers generally commented that their second swim was faster “There must be a mistake in timing. I found it much easier this time even though I took longer”. Swims also felt more comfortable “Generally I felt better all around.” Comments from the disassociators implied that the second swim was more enjoyable. The BIS “gave me other things to think about. I was not as mentally drained prior to the swim as I was in the first swim”. Subjects favoring the first swim (100% associative) attributed it to physical and mental factors. For instance, one subject suffered from a headache during the second swim and another blamed it on exhaustion because of work-out before the second swim. Also, one swimmer commented on “feeling more relaxed” and being less stressed during the first swim.
DISCUSSION
These results suggest that distance swimmers prefer associative thinking when swimming. Similar results were found in other studies with marathon runners during races (Masters and Lambert, 1989; Morgan and Pollock, 1977). Elite distance runners were found to be mostly associative thinkers throughout important races. Their results encouraged researchers to consider the notion of “the better the associative thinking the better the performance” (Schomer, 1987). Yet in this study, swimmers did not significantly improve their swimming times even after having read the BIS for an associative strategy. The strong preference for swimmers’ associative thinking was reflected mostly in the middle of the swim rather than throughout the entire swim. In comparison to distance runners during important races, the participants did not perceive the swim to be a race. Interestingly, a difference was found in muscular fatigue after the second swim despite the similar timed performances, RPE and heart rates between both swims. Three recommendations are suggested. Different results were found by Rushall and Shewchuk (1989). They found that thought content instructions improved swimming workout performance in at least two of the three thought conditions. In future studies, the extent to conformity of the BIS should be examined. Secondly, an 800 meter swim may not have been far enough for distance swimmers to use dissociative strategies especially since the groups’ average swimming per week was 4,490 m. Finally, the 800 m swims may have been too familiar for the participants, knowing their pace and the approximate time required. Perhaps, time could be a better independent variable than distance.
References
Borg, G. (1982). Psychophysical Bases of Perceived Exertion. Medicine and Science in Sports and Exercise, 14, 337-381.
Daniels, F.S. and Landers, D.M. (1981). Biofeedback and Shooting Performance: A Test of Deregulation and Systems Theory. Journal of Sport Psychology., 4, 271-282.
Gill, D.L., & Strom, E.H. (1985). The Effect of Attentional Focus on Performance of an Endurance Task. International Journal of Sport Psychology, 16, 217-223.
Koltyn, K. F., O’Connor, P. J., & Morgan, W. P. (1991). Perception of Effort in Female and Male Competitive Swimmers. International Journal of Sports Medicine, 12, 427-429.
Masters, K.S., & Lambert, M.J. (1989). The Relations Between Cognitive Coping Strategies, Reasons for Running, Injury, and Performance of Marathon Runners. Journal of Sport & Exercise Psychology, 11, 161-170.
Morgan, W.P. (1978). The Mind of the Marathoner. Psychology Today, April, pp. 38-40,43, 45-46, 49.
Morgan, W. P., Costill, D. L., Flynn, M. G., Raglin, J. S., & O’Connor, P. J. (1988). Mood Disturbances Following Increased Training in Swimmers. Medicine and Science in Sports and Exercise, 20, 408-414.
Morgan, W.P. & Pollock, M.L. (1977). Psychologic Characterization of the Elite Distance Runner. Annals of the New York Academy of Sciences, 301, 382-403.
Padgett, V.R., & Hill, A.K. (1989). Maximizing Athletic Performance in Endurance Events: A Comparison of Cognitive Strategies. Journal of Applied Social Psychology, 19(4), 331-340.
Pennebaker, J.A. & Lightner, J.M. (1980). Competition of Internal and External Information in an Exercise Setting. Journal of Personality and Social Psychology, 39, 165-174.
Pennebaker,J.A. & Skelton, J. (1978). Psychological parameters of Physical Symptoms. Personality and Social Psychology Bulletin. 4,524-530.
Rushall, B. S., & Shewchuk, M. L. (1989). Effects of Thought Content Instructions on Swimming Performance. Journal of Sports Medicine and Physical Fitness, 29, 327-334.
Sewell, D. F. (1996). Attention-focusing Instructions and Training Times in Competitive Youth Swimmers. Perceptual and Motor Skills, 83, 915-920.
Schomer, H.H. (1987). Mental Strategy Training Programme For Marathon Runners. International Journal of Sport Psychology, 18, 133-151.
Schomer, H.H. (1986). Mental Strategy and The Perception of Effort of Marathon Runners. International Journal of Sport Psychology, 17, 41-59.
Weinberg, R.S., Smith, S., Jackson, A. & Gould, A. (1984). Effect of Association, Dissociation and Positive Self-Talk Strategies on Endurance Performance. Canadian Journal of Applied Sports Science, 9(1), 25-32.
Correspondence concerning this article should be addressed to Dr. Roger T. Couture, School of Human Kinetics, Laurentian University, Sudbury, Ontario, Canada, P3E 2C6; Tel.# (705) 675-1151, ext. 1023.E-Mail: Rcouture@NICKEL.LAURENTIAN.CA
This study was supported by a grant from the Laurentian University Research Fund, Sudbury, Ontario, Canada.
During the past several years we have learned a lot about the effects
of strength training and body composition. For example, a carefully controlled
study at Tufts University showed significant changes in body composition
from a basic program of strength exercise (Campbell et al. 1994).
The subjects added three pounds of lean weight, lost four pounds
of fat weight, increased their resting metabolic rate by seven percent and
increased their daily energy requirements by 15 percent after 12 weeks of
strength training.
Research with over 1100 previously sedentary adults revealed similar
body composition improvements from eight weeks of standard strength training
(Westcott and Guy 1996). The program participants increased their lean weight
by 2.4 pounds and decreased their fat weight by 4.6 pounds.
Of course, unfit individuals tend to improve their body composition
at faster rates than people who are presently doing strength exercise. Many
people want to know if strength training can further enhance body composition
in well-conditioned exercisers.
Previous studies have demonstrated that various high-intensity training
techniques are more effective than standard training protocols for increasing
muscle strength in both beginning and advanced participants (Westcott 1996,
1997a, 1997b; Westcott and La Rosa Loud 1997). As shown in Figures 1 and
2, slow training produced greater strength gains than standard training for
both beginning and advanced trainees. As illustrated in Figures 3 and 4,
breakdown training resulted in greater strength gains than standard training
for both beginning and advanced exercisers. Likewise, assisted training generated
greater strength gains than standard training for both beginning and advanced
subjects (see Figures 5 and 6).
We have recently examined the effects of combined high-intensity
training techniques on body composition changes in well-conditioned participants.
The six-week advanced exercise program included slow training, breakdown
training, assisted training, and pre-exhaustion training. The 48 subjects
added 2.5 pounds of lean weight and lost 3.3 pounds of fat weight as a result
of their training efforts, which represented more improvement than we expected
from regular strength exercisers.
We have been pleased with our participants’ positive response to
the combined approach of high-intensity strength training techniques. Our
standard exercise protocol is outlined in Table I.
We observed that many program participants selected the pre-exhaustion
technique for their sixth week of high intensity training. Although we do
not have data that show this training method to be better than the others,
there may be some benefit in performing more pre-exhaustion sessions.
Psychologically, changing exercises at the point of muscle fatigue may be
more appealing than performing more repetitions of the same movement pattern
with less weight or with manual resistance. Physiologically, performing two
different exercises for the target muscle group recruits more muscle fibers
which may enhance the training stimulus. In addition to more exercises,
pre-exhaustion programs require more training time and may therefore be the
best high-intensity technique for burning calories.
Table I: Standard Exercise Protocol
Week Days
Training Technique
Total Exercises
Total Time
1. M & F
Breakdown
(10 reps to fatigue
plus 3 reps with
10-20% less weight)
12
20 Minutes
2. M & F
Assisted
(10 reps to fatigue
plus 3 reps with
manual assistance)
12
20 Minutes
3. M & F
Slow Positive
(5 reps to fatigue
with 10 seconds lifting
and 4 seconds lowering)
12
20 Minutes
4. M & F
Slow Negative
(5 reps to fatigue
with 4 seconds lifting
and 10 seconds lowering)
12
20 Minutes
5. M & F
Pre-Exhaustion
(10 reps to fatigue with
first exercise plus 5 reps
with second exercise)
16
25 Minutes
6. M & F
Personal Preference
(Trainee chooses the
technique that seemed
most productive)
12-16
20-25 Minutes
As many of our intermediate level strength trainees want to improve
their body composition, we presently provide high-intensity training programs
with more emphasis on pre-exhaustion techniques (Table II). The results are
encouraging, but we try to be cautious about overtraining. Our members seem
to respond well to six weeks of high-intensity training followed by six weeks
of standard training to maintain their new level of strength and
fitness.
Although we have not previously provided nutritional counseling to
our high-intensity training participants, this would undoubtedly be beneficial
for clients who want to lose fat as well as build muscle. A combination of
individualized high-intensity strength exercise and sound dietary guidelines
should produce significant improvements in body composition.
Table II: High Intensity Training Techniques
BASIC DESCRIPTIONS
Name
Procedure
Example
Comments
Breakdown Training
Perform about 10 reps
to fatigue with standard
weightload. Immediately
reduce resistance 10-20%
and perform about 3
more reps to second
level of fatigue.
Complete 10 leg
extensions with 150
lbs., then 3 more reps
with 120 lbs.
Change resistance
as quickly as possible
to maximize the
training effect.
Assisted Training
Perform about 10 reps
to fatigue with standard
weightload. Trainer
assists with 3 post
fatigue reps on lifting
phase only.
Complete 10 leg
extensions with 150
lbs., then 3 more reps
– with manual assistance
from trainer.
Assistance is given
only on the positive
muscle action where
it is necessary, but not
on the stronger nega-
tive muscle action
when it’s unnecessary.
Slow Positive Training
Perform about 5 reps
to fatigue with 10% less
than standard weight-load,
taking 10 seconds for each
positive muscle action and
4 seconds for each negative
muscle action.
Complete 5 leg
extensions with
135 lbs., counting
10 secs up and 4 secs
down for each rep.
Be sure to breathe
continuously
throughout
every repetition.
Slow Negative Training
Perform about 5 reps
to fatigue with 5% less
than standard weightload,
taking 4 seconds for each
positive muscle action
10 seconds for each
negative muscle action.
Complete 5 leg
extensions with
142.5 lbs., counting
4 secs up and 10 secs
and down for each rep.
Use smooth and
continuous move-
ments, rather than
choppy stop and
go movements.
Pre-Exhaustion Training
Perform two successive
exercises for target muscle
groups, typically a rotary
exercise followed immed-
iately by a linear exercise.
Use 10 reps to fatigue in
the first exercise and 5 reps
to fatigue in the second.
Complete 10 leg
extensions with
150 lbs., then 5 leg
presses with 300 lbs.
Take as little time
as possible between
the two successive
exercises to maximize
the
Table III: Examples of Pre-Exhaustion Exercise Combinations
1. Leg extension followed by leg press.
2. Leg curl followed by leg press.
3. Dumbbell lunge followed by barbell squat.
4. Dumbbell fly followed by barbell bench press.
5. Dumbbell pullover followed by lat pulldown.
6. Dumbbell lateral raise followed by dumbbell press.
7. Dumbbell curl followed by chin up.
8. Dumbbell overhead extension followed by bar dip.
Wayne L. Westcott, Ph.D., is fitness research director at the South
Shore YMCA in Quincy, MA. Dr. Westcott has written the Muscular Strength
And Endurance chapter for the ACE Personal Trainer Manual and has authored
several textbooks on strength training.
References
Campbell, W., M. Crim, V. Young & W. Evans. (1994). Increased
energy requirements and changes in body composition with resistance training
in older adults. American Journal of Clinical Nutrition, 60:
167-175.
Westcott, W. (1996). Strength training for life: Make your method
count. Nautilus Magazine, Spring 5: 2, 3-5.
Westcott, W. and Guy, J. (1996) A physical evolution: Sedentary adults
see marked improvements in as little as two days a week. IDEA Today 14:
9, 58-65.
Westcott, W. (1997a). Research: Research on advanced strength training. American Fitness Quarterly, 15: 4, 15-18.
Westcott, W. (1997b). Strength training 201. Fitness Management,
13:7, 33-35.
Westcott, W. and La Rosa Loud, R. (1997). A better way to beef up
strength workouts. Perspective, 23: 5, 32-34.
Submitted by: William L. Carroll, Ed.D., ATC, and Augustin Mendoza, M.D.
Training for Optimal Performance
Soccer is a major sport for young athletes in the United States, and is also rapidly becoming a major sport for males and females for all ages. Because young athletes go through puberty at different times, they vary a great deal among each other in size and maturity. These differences pose a challenge to the athletes and their coaches. The primary characteristics of a young athlete are: motivation; physical fitness (i.e. muscle strength, power, endurance, flexibility, proper body composition, and cardiac respiratory endurance); discipline, coachability; skills; ability to be a part of a team; ability to think under stress; and good spatial orientation.
The practice sessions for soccer should seek to achieve: physical conditioning, repetitive training, proper intensity of training, flexibility, and awareness that the achievement of proper endurance for the soccer athlete requires 4-6 months of training. Also, the coach should be aware that extreme and severe high intensity and high frequency training causes damage to muscle tissues and is counterproductive to the goals of the athlete. The pre-game meals should primarily be composed of carbohydrates, and balanced meals should be eaten prior to game days. Water consumption (hydration and rehydration) should be strongly encouraged with water breaks built into the training schedule and water available upon demand.(2)
Physiological and Chronological Age
Any middle school teacher can tell you that adolescent teenagers are difficult to handle and that they vary a great deal in size, height and maturity. This is because teenagers, in addition to possessing the normal genetic inheritance of size from their parents, are also in a very fast growth period (puberty). The growth spurt on the average is around 12 years of age for girls and 14 years of age for boys. Young athletes are experiencing a turmoil period which affects them both physiologically and hormonally. Therefore, young athletes come to soccer with these inherent and at times large differences in size, shape, height, and skill level. Because of these differences, it is very difficult to mold a team at this age group into a skilled unit.
Characteristics of a Soccer Player
All of the following player characteristics need not be present before the individual plays soccer. However, the individual should either show aptitude or at least a willingness to acquire these characteristics.
1. Motivation
The soccer player should be interested and motivated to play the game of soccer (i.e. kicking a ball, running, passing a ball, etc.). In other words, the player is receiving an enjoyment out of performing these tasks especially when it is performed spontaneously and without adults forcing them to do so.
2. Physical Fitness
The term physical fitness connotes different meaning for different activities. In the
context of soccer, it is the ability to play soccer for 60-90 minutes without fatigue, exhaustion, or other malsymptoms of a sedentary person. The player should have the following physical fitness characteristics to play soccer:
a. muscle strength and power
b. endurance
c. flexibility
d. proper body composition
e. cardiac respiratory endurance
3. Discipline
The ability to practice and play the game in a repeated fashion several times a week.
4. Coachability
The ability to take instructions and to try to comply with these instructions.
5. Skills or ability to learn skills
The ability to conduct or learn individual soccer skills with the ball such as kicking, receiving, passing, shooting, control, etc.
6. Ability to play in a team sport
The ability to cooperate with other team members to achieve a difficult task. Also, the player should have the ability to accept less personal recognition for the sake of the team. The player also should be able to associate with others for a long time and sometimes under stressful conditions. Finally, the player should have the ability to enjoy himself with others.
7. Ability to think under stress
Most people are not as logical under stressful conditions as they are normally. However, the well trained soccer player learns what to do under the various game conditions, and also learns to think quickly under stressful conditions.
8. Good Spatial Orientation
The ability to think and visualize in three dimensions and to be relevant to the soccer field is difficult for very young players. The player should be able to learn to adapt to the spatial orientation within the field and re-position himself/herself relevant to the ball, teammates and the opposing team members.
Practice Sessions
The purpose of this article is not to suggest specific exercises. There are other sources for the numerous soccer practice sessions. However, we will give a general outline that all soccer practice sessions should fall within. In this manner, each coach can use their creativity to make soccer practices more enjoyable and more beneficial to the different needs of the varied groups.
The practice sessions should be designed to make the individual a better soccer player. The best practice for any sport is to play that sport repeatedly in order to develop those muscles, skills, endurance, etc….., for that sport. It is a common occurrence for those who play one sport and then suddenly play another sport to have muscle aches after the first few times of the new sport. This is because they have used a different new set of muscles than they used before. This is called specificity of training. So, the more the soccer player plays soccer, the better he/she will become. This is not to say that the soccer game should not be broken down to small segments so that it can be taught and repeatedly reinforced.
In order to prepare the individual to play soccer, players and coaches should observe the following factors:
1. Physical conditioning
Increased ability to sustain both aerobic and anaerobic exercises.
2. Frequency of training
This should be 2-3 times a week for youngsters and 3-4 times a week for adults.
3. Warm-up
Static stretching should last 10-30 seconds and be repeated 3-5 times. Each stretching exercise should include a larger range of motion than the previous one. In addition, after each rigorous practice session, there should be 10 minutes of low to moderate cool-down exercises. Examples of cool-down exercises in soccer are individual skill exercises; jogging lightly, and best of all just walking or dribbling the ball lightly.
4. Time to peak endurance
Quick and severe training for 2-3 weeks prior to a season as is the case in some high schools after sedentary summer, cannot achieve endurance and may be detrimental to the athlete. This is because adaptation of the cardiorespiratory system and muscle enzymes require about six months of training to reach peak endurance capacity. Moreover, it takes 2-4 weeks without training (as may be the case during the summer for high schoolers) to lose most of endurance parameters (see section on endurance for details). Therefore, a well-planned long training period is an essential part of preparing players for the season.
5. Muscle Strength and Power
The use of moderate weight lifting for young athletes to increase strength and power in moderation is an acceptable form of exercise. Weight bearing exercises for children below 13 years of age is not recommended in the standing position where there is a great deal of compression force on the legs. In order to increase muscle strength, the muscle should be challenged by at least 60% of the maximal weight lifted the first time. Furthermore, in subsequent days and weeks, the muscle must be challenged by increasing weights, with high frequency repetition. Remember, an increase in muscle strength is not necessarily associated with a large increase in size of the muscle. Low frequency repetition increases the size of the muscle (body building) rather than increasing the muscle strength. While defenders may be able to use a greater muscle mass and strength, other soccer players need to increase strength more than muscle size in order to keep their agility and speed.
Soccer is a mixture of aerobic and anaerobic sport. Therefore, the training session should combine both modes. Aerobic (like marathon running, jogging, etc…) sessions are usually composed of slow rhythmic exercises. These exercises allow the body to utilize oxygen to burn foodstuff to produce the energy needed. Therefore, the best soccer training sessions should resemble match-like conditions which involve both anaerobic and aerobic exercises. These conditions consist of the player performing, for example, the following tasks:
(a) Aerobic exercises such as continuous jogging to re-position to a new ball position lasting 1-5 minutes. Repetition of this action 10-50 times per game.
(b) Anaerobic exercises such as sprinting — lasting from a second to 1 min. Repetition of this action 10-50 times per game.
(c) Midfielders do most of the jogging and sprinting throughout the game since they must perform offensive and defensive tasks.
(d) Defenders tend to do mostly jogging and less sprinting.
(e) Offensive players do more sprinting than jogging.
The details of the sessions should be left to the creativity of the coach to combine multiple game-drills that benefit the most for a given player and team.
Usually young players play more than one position (i.e. offensive versus defensive position). However, as the young players pass puberty, they become more specialized in a given general position. Therefore, each position may require slightly different emphasis. For example:
(a) Offensive players do mostly sprinting than jogging and therefore would require more anaerobic process adaptation.
(b) Defensive players tend to do mostly jogging and less sprinting and therefore would require more aerobic process adaptation.
(c) Midfielders tend to do both sprinting and jogging throughout the game since they must perform both offensive and defensive tasks. Therefore, midfielders would require an intensive training to adapt to both aerobic and anaerobic processes.(1)
Interval Training
The soccer player can benefit from interval training. Interval training consist of work bouts with rest intervals of ratio varying from 1:3 to 1:1 (work/rest) depending on the need and the physical fitness of the individual. The work period can lasts a few seconds up to several minutes. The whole cycle can be repeated 5-20 times. A short high intensity (sprinting) work bout lasting greater than 15 seconds can improve the anaerobic system with rest period of 30 seconds. Interval training to improve the aerobic system could consist of ratio’s of 1:1 or 1:1:5. The exercise period could last 60-90 seconds in order to force oxygen consumption followed with a recovery period varying from 60 seconds up to 135 seconds.(2)
Circuit Training
Circuit training attempts to use economically time of exercise to improve strength, power and cardiorespiratory system. Work sessions should combine resistance, speed and rest. For example, working periods can vary from 30-60 seconds with similar rest periods. The number of different stations could be as high as 15 stations of differing exercises.(2)
Preparations for the Soccer Season
Physical Fitness Assessment
1. Physical Exams and Screening
2. Physical Fitness Tests
a. Cardiorespiratory endurance
1. Heart rate recovery test
2. Step test
3. Running
4. Walking
b. Body Composition
1. Anthropometric test
2. Skinfold test
c. Muscle Power and Strength
d. Flexibility
Prevention of Injuries
a. Proper Preparation of teens and players
b. Equal Competition
c. Proper rules and refereeing
d. Proper sequence of warm-ups, stretching, and exercises
Protective Gear in Soccer
1. Cleats
2. Shin Guards
3. Mouth protector (for persons with orthodontics)
4. Goalies outfit (elbows, knees, and hip cushion)
5. Taping (when necessary)
Water and Electrolyte Balance
Water is the most important and critical nutrient to the survival and well being of a person. One can survive without intake of other nutrients for days, weeks, and even months but one cannot survive without water for more than a few days. In a 70 Kg person, the water content is about 40 liters (i.e. 60% of body weight). Most of the water (25 liters) is inside cells of the body and about 15 liters lie outside the cells. The blood volume is about 5 liters and the maintenance of this volume is critical to the survival of the person. For example, daily fluid intake can vary from 1-7 liters, while the blood volume must remain constant. Excess fluid intake can easily be regulated; however, a problem. arises when fluid intake is below one liter per day and blood volume starts to become lower than 5 liters (for example about volume of 4 liters and below can cause death). Under sedentary conditions skin and kidney (i.e. urine output) are the most important regulators of body water. Under the conditions of hot weather and exercises (despite fluid intake in many cases, the skin (sweating) becomes the only important regulator of body water as well as the body temperature. The daily loss of water in a heavy, prolonged exercise (3 hours marathon) can increase from 0.1 to 5 liters.(6)
Sweating is absolutely necessary in order to maintain constant body temperature. The sweat rate usually corresponds to increases in energy expenditure by the athlete. Trained athletes have a more sensitive sweating system than non-athletes due to adaptation by the repetitive exercises. Of the 5 liters of H2O, a marathon runner’s losses (despite fluid intake in many cases) represent 12% of body water and 8% of body weight. Anything above 2% weight loss due to exercise induces severe demands on the thermoregulatory and cardiovascular systems.
All of the energy expenditure during exercise ends up as heat. Therefore, body temperature will rise rapidly during exercise if cooling due to sweating is not functioning. The prolonged increase in body temperature will eventually cause serious damage to the thermoregulatory system, which can result in serious damage to the brain — the most sensitive organ. Thirst, unfortunately, is not a reliable indicator during exercise (i.e. under any stressful conditions). Therefore, athletes should drink water not just to quench their thirst, but as part of their exercise regime. Figures 3 and 4 represent a hypothetical daily water output and water intake for persons who are: sedentary, a marathon running for 3 hours, or soccer players (90-100 minutes). The numbers are rough estimates, and for illustration purpose only. The most scientific way to determine how much water intake ought to be is to weigh the player before and during the game. The loss of weight due to water loss should be adjusted by drinking the same amount of water. Remember, it is better to drink more than less water.
Children utilize a greater metabolic energy and thus produce more heat than adults to perform the same task. Fortunately, children dissipate heat better than adults due to a larger surface area to mass ratio than adults. However, when ambient temperature is hot and humid, the dissipation of heat is inhibited and thus children maybe at a greater risk than adults during exercise.
Electrolytes such as Na+, K+, Cl-, Ca2 and Mg2+ are the most important ions and their amount in the cell and the blood is critical in maintaining normal body function. As we sweat more during exercise, the amount of these ions in the sweat is less than that of the blood. In other words, the body is losing more water than ions. Under heavy exercise conditions, the body loses about 5-7 grams sodium chloride. However, there is a minimal loss of K+ and Mg2+. Under conditions of continued exercise (up to 80-90 minutes) there is a need to replenish water continuously, but not salt. If there is heavy exercise beyond the 80-90 minutes, salt replenishment is appropriate. The use of salt tablets during the early phase of exercise (in most cases of soccer) is detrimental to the body. The body fluid has a higher salt concentration after exercise than before; therefore, the body needs pure water to bring the blood composition back to normal levels.(6)(2)
Heat Related Illnesses
Heat Cramps
They are similar to other muscle cramps, which may be due to: sudden blows; over exercise; lack of blood supply, etc.
Cause: Reduced blood flow to the muscle due to: loss of water, prolonged loss of minerals, etc.
Symptoms: Spasmodic tonic contraction of a given muscle.
Onset: Gradual or sudden.
Danger: None if treated. Heat cramps could lead to termination of that particular exercise for a few days.
Prevention: Proper physical fitness, proper warm-ups and stretching exercises prior to the activity and temporary termination of activity.
Treatment: Termination of activity. Stretching, rest and ice treatment necessary.
Heat Exhaustion
Cause: Loss of water.
Symptoms: Tiredness, weakness, malaise, and progressively weaker.
Onset: Gradual and over several days.
Danger: The player may go into shock because of reduced blood volume This rarely happens, however, as it is not an emergency condition.
Prevention: Proper physical fitness and proper hydration before and during the exercise and termination of activity.
Treatment: Cooling, drink water, and later drinking large amounts of mineral rich fluid such as fruit and vegetable juices.
Heat Stroke
Brain cells in the hypothalamus maintain body temperature close to 98.6oF. These cells respond to the blood temperature that passes through them. The cells regulate the skin by sending signals to release skin vasodilator in order to increase sweating. When rectal temperatures reach 41oC – 43oC, unconsciousness may develop; if that happens, the mortality rate ranges from 50-70%. Heat stroke is the second cause of death among athletes.
Cause: Loss of water and sudden uncontrolled rise in body temperature due to the failure of the thermoregulatory center in the brain.
Symptoms: It is a Medical Emergency. May lead to death or irreversible damage. Person shows behavioral or mental status changes during heat stress. These symptoms include: sense of impending doom, headache, dizziness, confusion and weakness. Symptoms that could lead to heat stroke are:
a. high temperature and high humidity
b. high rectal temperature
c. hot dry skin
d. cardiorespiratory and central nervous system disturbances
e. clouded consciousness and finally collapse
Onset: Sudden
Danger: Brain damage and death is imminent if not treated quickly.
Prevention: Proper physical fitness and proper hydration before and during the exercise and termination of activity.
Treatment
1. Call for an ambulance.
2. Remove clothes and cool with ice and cold water on the body.
3. Monitor vital signs. (i.e. breathing, heart beat, pupil size).
4. Massage extremities to promote cooling.
5. Once the body temperature cools and the person is quite alert, remove from cold environment to prevent hypothermia.(3)
In the hospital they may perform the following:
1. Administer I.V. fluid (1400 ml for first hour).
2. Monitor urinary output – Mannitol may be given to promote urination.
3. Digitalis may be considered for heart failure.
4. Isoproterenol administration to increase cardia output (if needed).
5. Oxygen may be given.
6. Other procedures as necessary may be used.
7. Continue to monitor kidney and brain functions.
Adaptation of Endurance Training
Endurance training connotes a process of adaptive changes to achieve the strength, power and cardiorespiratory capacity to complete the specific physical task. Endurance training requires several months of rhythmic and continued exercise that results in an increase in the body’s number of capillaries, maximal oxygen uptake, stroke volume, and enzymes. Moreover, endurance training increases the sectional size of slow type fibers and there is an actual conversion of fast type fibers (Type 11B.) to slow (Type 11A.). The Type 11B. fibers are the fast fibers, and are capable of lasting longer than the type 11A. fibers. Therefore, there are major underlying biochemical changes in the various organs and cells involved in the physical activity that provides the needed energy, strength and power to carry out the task. Soccer requires a combination of slow and fast fibers because soccer playing is a combination of quick actions lasting less than 1-2 minutes and a prolonged activities which can last 5-10 minutes.
Athletic physical conditioning has become a very serious and scientific endeavor. In the past 20 years, there has been an increase in our understanding of the physiology and biochemistry of exercise. There has also been an increase in interest in the mechanism of how exercise induces physiological and biochemical adaptation at the cellular and organismic level and how this accounts for the improved performance of athletes in a given sport.(1)
Endurance in sports means the ability of the person to perform a specific prolonged exercise or work to achieve a reasonable task without adverse reactions such as fatigue, exhaustion, and injury. Endurance can mean different things for different tasks (i.e. sport activity), as each task may involved unique muscle groups and skill levels. Therefore, there are several components of endurance that develop differentially during endurance repetitive training for the specific sport. The components of endurance are: muscle strength and power, the cardiovasculatory system, and the respiratory system. The cardio-respiratory endurance is needed with varying intensities in all sports. However, strength and power can vary in magnitude from muscle to muscle. Therefore, local endurance is quite important for a given sport. During endurance training of repetitive exercise for several months, the muscles adapt to generate force and to maintain a supply of energy. The key factor in endurance training is the exertion of physical stress with certain frequency and for lengths of time. This chronic muscular activity stimulates growth of the muscle as well as the development of endurance in terms of oxygen delivery, energy production, and permanent metabolic and structural changes. Therefore, endurance training in this context is a low-level, prolonged-intensity aerobic training exercise where the system can utilize oxygen as the initial trigger of energy source. The first general aspect of endurance adaptation is the adaptation of the cardiovascular/respiratory system to accommodate the increased frequent demand for oxygen uptake and delivery.
Cardiovascular – Respiratory Adaptation
Rhythmic and continued exercise requires a greater use of oxygen at the muscle site. Therefore, the routes of uptake and transport of oxygen from the air to muscle tissues must adapt to the increased rate of delivery and extraction. A measurement of cardiorespiratory endurance is the VO2 max. VO2 max is the maximal oxygen uptake during the maximal exercise, and it differs from person to person. In order to compare exercise-related data from person to person, the data is expressed relative to a specific level of intensity of exercise and represented as expressed as a percent of VO2 max. To illustrate its importance, endurance training can change the VO2 max by as much as 20%. This is the first indication that true structural and biochemical changes must occur in order to metabolize the increased oxygen uptake. The first apparent result of an exercise is the immediate increase in heart rate. The resting rate is 80 beats per minute; however, during exercise the heart rate can go as high as 190 beats per minutes. After several months of endurance training, heart rates can go as low as 40 beats per min. This reflects several factors of adaptation to exercise among them being the autonomic nervous system. However, the one aspect related directly to the heart rate is the fact that despite the lowered heart rate, the heart provides a greater cardiac output because the stroke column increases by as much as 80%. In a highly trained athlete, the refilling is more complete. More importantly, the left ventricle strength and power is dramatically increased. The left ventricle undergoes hypertrophy with endurance training, which means the actual heart muscle mass and volume are increased. Heart size is greater in endurance trained athletes by as much as 25%, as compared to a sedentary person. Moreover, the contraction of contractile proteins are increased and the composition of the protein changed. Also, oxygen delivery of the blood supply to the heart is improved because the number and size of capillaries per cross-sensational areas of muscle increases by as much 50% due to endurance training. Endurance training also improves (by as much as 80%) the muscle content of myoglobin. Myoglobin carries oxygen within the muscle tissue. These dramatic biochemical adaptations in the oxygen delivery system parallels those of the heart and thus complements the entire scope of the biochemical adaptation for a better performance by the trained athlete.(2)
Blood Volume and Composition
There are three major changes in the blood due to endurance training: (1) increased blood volume; (2) increased hematocrit (i.e. increase in the total number of red blood cells (RBC); and (3) decrease in viscosity. The increased blood volume is as high as 20%. However, the increase in RBC is less pronounced and as a consequence the viscosity of the blood decreases. The increase in blood volume is the key important factor for an endurance trained athlete. The increased blood volume enhances O2 delivery as well as enhancing microcirculation. The increase in microcirculation is even more pronounced due to the blood’s reduced viscosity. A trained athlete also has another advantage in greater capacity to clear lactate from the muscle and utilizing lactate as an energy substrate. Thus, the level of blood lactate in a trained athlete is lower than in a sedentary person. This phenomenon is referred to as a lactate shift. A trained athlete therefore has a greater endurance with less fatigue and cramps due to decreased levels of blood lactate.
Common Injuries Encountered in the Sport of Soccer
The physiological principles of tissue damage and tissue healing are essentially the same for all sports. What makes each sport somewhat unique in terms of the injuries encountered is the specific sport activities which lead to specific mechanisms of injury. The soccer skills involved with passing and dribbling, kicking, ball control, heading, tackling and goal keeping all, when combined with the principles of force, gravity, ground contact, and torque, can lead to injuries.
Unfortunately and wrongly, our youngest athletes (such as youth soccer players) receive the least sports medicine coverage. Therefore, injury recognition and evaluation becomes the premise of the coach or parent who may have little or no preparation for the task.
In an attempt to simplify the evaluation procedures, the most basic acronym, HOPS, should be employed. HOPS stands for history, observation, palpation and strength/sensation. This primitive evaluation system may be utilized with any type of injury.
A good preparticipation physical examination is mandatory. This provides the benchmark from which deviations from the norm may be measured. A good preparticipation physical should minimally include a medical history, height and weight check, visual acuity check or screen, orthopedic or joint evaluation and visceral examination. Physicians specializing in sports medicine are the best sources for these physical exams.
Observation begins the first time one sees the injured athlete. Is he/she conscious, does the athlete walk with an antalgic gait, does the athlete hold any body part as a protective manner, and is the athlete visibly exhibiting pain? These are all important observational factors. Also, if one is dealing with an extremity injury, the evaluator should visibly compare that limb to the contralateral or uninjured limb.
Palpation involves touching and moving the injured body part. If pain is diffuse, palpation may be of limited value. However, if the pain is specific or point tender, then active, passive and resitive motion will assist the evaluator in localizing the injury site or injured structure.
Strength/sensation is the final aspect of the field evaluation. Again, if dealing with an extremity injury, one has the luxury of being able to compare strength and sensation of the injured limb to that of the uninjured.
Common injuries encountered in the sport of soccer include:
Sprains: A sprain represents damage to a ligament. Common sprain sites include the ankle, knee and wrist.
Strains: A strain represents damage to a musculotendinous unit. Common strain sites encountered in soccer include the gastrocnemius, quadriceps, hamstring, low back and shoulder.
Fractures: Common fracture sites include the fingers, tibia, fibula, radius and ulna. These fractures are usually resultant from falls. The only method of positive fracture diagnosis is X-ray.
Dislocations: Dislocation sites commonly encountered may include fingers, should and elbow. The most common mechanism of injury resulting in a dislocation is the fall on the outstretched hand or arm.
Contusions: Contusions are resultant from contact with the ball, with other players, or with the ground.
Concussions
When does an injury need to be referred to a physician? Although this is a difficult question to answer, the following guidelines will assist the layman in making the decision:
1. Suspicions of a fracture
2. Suspicions of a concussion
3. An injury in which the pain cannot be controlled with conservative measures
4. A laceration that may require sutures
5. Any suspicion of internal injury
Additionally, any time the layman is unsure of his/her evaluation, the athlete should be referred to a physician.
Conservative Care of Acute Injuries
The acronym PRICE represents a form of conservation care for acute injuries.
“P” stands for protection. An ankle injury can be protected by placing the athlete on crutches non-weight bearing.
“R” stands for rest. Rest means not using the injury body part and allowing it to heal properly.
“I” stands forice. Ice or cold is utilized in cryotherapy. The use of ice results in a greater chance of tissue survival, reduces degradation of healthy tissue, induces vasoconstriction which prevents further swelling and loss of range of motion and enhances early mobilization. Ice also acts as a topical anesthetic.
“C” stands for compression. Specific compression when applied to an extremity injury may prevent swelling and the accompanying loss of range of motion.
“E” stands for elevation. By elevating an extremity injury, once reduces effusion and dependent bleeding. Again, this reduces swelling and loss of range of motion, both of which tend to protract injury recovery time.
Remember, the whole idea behind the science of sports medicine is to provide the best possible environment for healing to occur.
Summary
Youth and age group soccer can be an extremely positive experiences for the young athlete. Skill development, coordination, socialization skills, and cooperation are all positive results of a healthy youth and age group soccer program.
In order to assure a healthy program, one must insist that sports medicine considerations such as preparticipation physical exams, proper conditioning, conservative injury care and warm- up and cool down periods are observed as well as adequate hydration and rehydration.
Submitted by: Jamie Nelson, Daniel R. Czech, A. Barry Joyner, Barry Munkasy & Tony Lachowetz
ABSTRACT
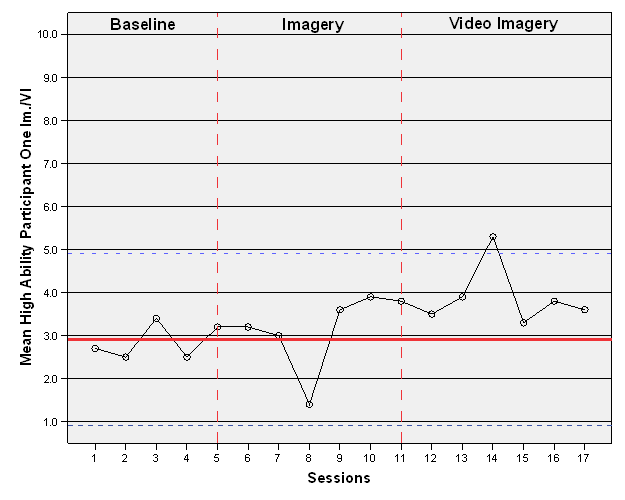
The purpose of this study was to examine the effects of a three-week imagery and video imagery intervention program on the throwing accuracy of individual baseball pitchers. A secondary purpose of this study was to investigate whether differences in accuracy response characterize both low- and high-ability imagers. A sample of pitchers (n=30) were asked to take the Movement Imagery Questionnaire–Revised; study participants were randomly selected from the highest and lowest 20% of the group. The participants were obtained from high school and college teams within southeastern Georgia (n= 6). Following the first week of baseline measurements, 2 high-ability and 2 low-ability imagers took part in a three-week video imagery and imagery intervention program. One participant from each group together constituted a control group, which was asked only to try their best when throwing for the study’s accuracy measurements. Results showed that 2 participants demonstrated an increase in performance, while all participants expressed a desire to continue to use imagery for its various effects. Suggestions for future research and further insight are discussed.
INTRODUCTION
Imagery has been shown to be very effective for improving accuracy in sport. Thomas and Fogarty (1997) found that imagery combined with positive self-talk improved not only putting performance, but psychological factors as well. Woolfork et al. (2005) found that positive imagery participants, in comparison to negative imagery training and control group participants, experienced significant increases in putting performance. Moreover, imagery has been shown to positively enhance free-throw shooting among collegiate basketball players. Kearns and Crossman (1992), Shambrook and Bull (1996), Templin and Vernacchia (1993, 1995),Stewart (1997), and Carboni, Burke, Joyner, Hardy, and Blom (2000) have determined imagery to be to some degree effective for most individuals at enhancing free-throw performance.
Much of the research cited above utilized a single subject design. This type of design has proved important in applied sport psychology, demonstrating improvement in individual cases that might be overlooked by traditional group analysis (Shambrook & Bull, 1996). For instance, when a multiple baseline design is used, a conclusion could be drawn that any effects were due to the specific intervention (Bryan, 1987, p. 286). The single subject design, in contrast, allows for individual analysis of the imagery implementation and a way to tailor the intervention to the individual (Stewart, 1997).
Visualization theories have not always been applied to sport performance; they began in the field of cognitive and spatial awareness research. Bess (1909) was among the first researchers of the topic and is credited with developing the measuring system for visualization. The Bess Scale addresses differences in individual imagery ability, drawing on cognitive theory of imagery and tied closely to the understanding of the term kinesthetic imagery(Schiffman, 1995).
A pitcher may be asked to imagine the ball in hand before a throw, to feel the laces and texture on the palm, maybe even to brush the dirt off, as if the ball was just grabbed from the ground. Bess notes that the image should be as clear and detailed as possible, and his Bess Scale measures the vividness of the visualizations practiced with seven classifications of vagueness and vividness. However, Wilson & Barber (1981) found that individuals can vary greatly in their ability to visualize, even when their Bess Scale scores are alike. Moreover, Stoksahl and Ascough (1998) also found that some athletes were very detailed in their imaging, while others were very vague; they concluded that the less vivid images may not be as effective for enhancing performance. Therefore, athletes with lower imagery ability may not reap full performance-enhancement benefits from imagery training. Such findings provide one more reason to investigate the effects of video imagery: Individuals who lack vivid imaging skills may find that a video re-enactment of the task allows them to see the desired performance very clearly, aiding mental preparation for an actual event or task demonstration.
Little research appears in the literature which has examined the effects on performance of internal video imagery, or video depicting an athlete’s internal perspective during performance. However, at least some research has integrated videotape modeling with imagery training. Hall and Erffmmeyer (1983) investigated female high school basketball players who were assigned to a video modeling/imagery group and a relaxation/imagery group. Results can only be attributed to a combination of psychological skills, as they were compounded within the study, but it was concluded that the video modeling/imagery group demonstrated better performance in foul shooting, compared to the relaxation/imagery group. Little research seems to exist exploring internal video imagery in other sports contexts, specifically baseball and, more specifically, pitching accuracy.
While general research on imagery is vast, this study seeks to investigate the effects of cognitive imagery and video imagery on one phenomenon: the throwing performance of baseball pitchers. A secondary purpose of this study is to see whether low-ability imagery and high-ability imagery are associated with distinct performance responses following video and cognitive imagery interventions.
METHOD
Participants
The study participants were 6 baseball pitchers from southeastern Georgia. They were selected from the region’s high schools and colleges. Four males, 2 current college athletes and 2 current high school athletes, took part in the study. The participants’ mean age was 19.8 years, with ages ranging from 16 to 22 years. Only athletes currently on pitching staffs of high school or college baseball teams were utilized. All participants had been baseball athletes for at least the previous 2 years, at either the high school or college level. All were asked to return a signed consent form before participating in the study; participants under 18 years of age were asked to return a parental consent form before participating. The consent form assured participants of confidentiality, briefed them on the study’s purpose, and listed the risks and benefits of participation. Contact was made with each institution, informing participants, parents, and coaches that athletes’ participation was completely voluntary.
Apparatus
A Samsung Sports Camcorder SC-X205L/X210L was used to record all accuracy-measurement sessions, in order to ensure that accurate points were recorded for each pitch. At no time, however, was the pitcher himself captured in these recordings. The Samsung Camcorder SC-X205L/X210L external helmet camera module, used to capture recordings of an accurate pitch from the internal perspective of the pitcher, was used in the video imagery interventions.
Prior to the study, an imagery ability test was given to a group of 30 high school and college baseball pitchers, to identify athletes with high- and low-ability imagery skills who might become part of the study sample. The Movement Imagery Questionnaire- Revised (MIQ-R) was used to measure the athletes’ imagery ability (see Appendix A). Hall and Martin (1997) developed the MIQ-R, a revision of Hall and Pongrac’s Movement Imagery Questionnaire, or MIQ (1983), in order to assess individuals’ capacity to generate visual imagery and also kinesthetic (or movement) imagery. The present researchers have determined the MIQ- R to be a valid and reliable revision of the original instrument: Earlier work has established significant correlations for the MIQ-R’s visual and kinesthetic scales. For the MIQ, Hall, Pongrac, and Buckholz (1985) obtained a test–retest co-efficiency score of .83; in terms of internal consistencies, a score of .89 was obtained for the visual scale and a score of .88 was obtained for the kinesthetic scale (Atienza et al., 1994).
A Post Study Imagery Questionnaire was distributed to the present study’s participants at the completion of the investigation. This questionnaire sought feedback from each pitcher as to prior experience with imagery, present attitude toward imagery, and likelihood of future imagery use. Moreover, it asked the athletes to think about effects of imagery occurring in dimensions other than performance. The questionnaire asked these questions, specifically: Did you at any time use imagery outside of this study? How do you feel about the use of imagery in general? Do you feel it helped you and how so? Do you feel there was a difference between the two types of imagery and if so what were they? Will you continue imagery use?
Procedures
The pitchers’ completed MIQ-R instruments; later on, their scores were collected and recorded by number, both to protect confidentiality and to help ensure random selection of participants. Pitchers completing the MIQ-R were also given a brief explanation of what the instrument covered and directions for providing answers. A 7-point Likert scale was employed for each question, and the points assigned each question were totaled for each participant. Using the scores obtained, 3 participants were chosen at random from the top 20% of scores, and another 3 were selected randomly from the bottom 20%; the 6 were asked to participate in the study. By omitting participants with middle-ranking scores, the study sought to secure a sample that truly represented high- and low-ability imagery skills. Participants signed a consent form or obtained written parental consent prior to participating.
Participants were asked to meet with an “observer” 5 times during the first week of the study, the period during which a stable baseline was to be established for each pitcher; after a baseline existed (which ideally required 1 week but in fact might have required more time), participant and observer were to meet 4 times during each of the next 3 weeks. The 3 weeks constituted the invention portion of the study. Prior to the intervention, each pitcher’s throwing performance was measured 5 times a week, until he had demonstrated a stable baseline, defined as an average score displaying no more than a 2-point variance in at least 3 consecutive trials. The first-week, baseline portion of the study was followed by imagery interventions beginning in the second week; each imagery intervention required 6 visits, or one and one-half weeks. Measurements were taken 4 times a week, post imagery session, during the imagery and video imagery intervention programs, until the study’s completion. Throwing-performance measurements were determined by averaging a pitcher’s scores for 10 pitches in the visitors bullpen of an NCAA Division I university. The measurement apparatus was placed in front of the bullpen home plate. During the baseline portion of the study, the Samsung Sports Camcorder SC-X205L/X210L was used to create video imagery segments for use during the intervention portion, with each pitcher wearing the “helmet-cam” module (placed aside his head, at eye level) and capturing his own internal perspective on the throwing of an accurate pitch. (At no time was any pitcher himself captured in a recording.) The module is worn comfortably on a headband, and no participate indicated discomfort during its use. The study design incorporated counterbalancing to eliminate sequence effects.
Participant 1 and Participant 4 experienced the cognitive imagery intervention during Week 1 of the intervention portion of the study, followed by video imagery intervention beginning in the middle of Week 2 (the two athletes’ seventh study session). Participant 2 and Participant 5 experienced video imagery sessions as the initial intervention during Week 1 of the study’s intervention portion. They participated in cognitive imagery intervention during Session 7 through Session 12. The throwing accuracy of Participant 3 and Participant 6 was measured 4 times a week, and they received no intervention, serving as a control group.
The university’s Mental Edge Training Facility was used for the video and cognitive imagery sessions, which were conducted individually (rather than in groups) during scheduled time slots. An imagery session was of a 10-minute (approximately) duration. During the video imagery interventions, participants were asked to watch the previously recorded 10-point pitch while imagining accompanying sensations, to include sounds, smells, tastes, and textures, in as much detail as possible. During the cognitive imagery interventions, in contrast, they were asked to imagine the 10-point pitch as vividly as they were able, again using the five senses as much as possible. At the study’s end, each participant completed the Post Study Imagery Questionnaire, providing insights into his attitudes towards imagery generally, as well as his unique responses to imagery practice, performance, or similarly related issue. The Post Study Imagery Questionnaire also attempted to determine whether and why players would continue to practice imagery techniques.
Data Analysis
Data were represented graphically to describe each participant, then reviewed for practical differences in throwing accuracy. Ocular statistics (Carboni et al., 2000) were reviewed by a group of trained researchers to determine actual changes in throwing accuracy and to provide control of the researcher’s bias. Qualitative results of the Post Study Imagery Questionnaire were collected and reported.
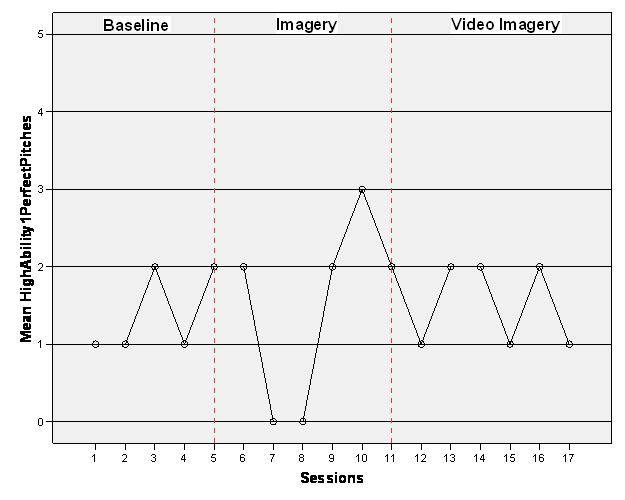
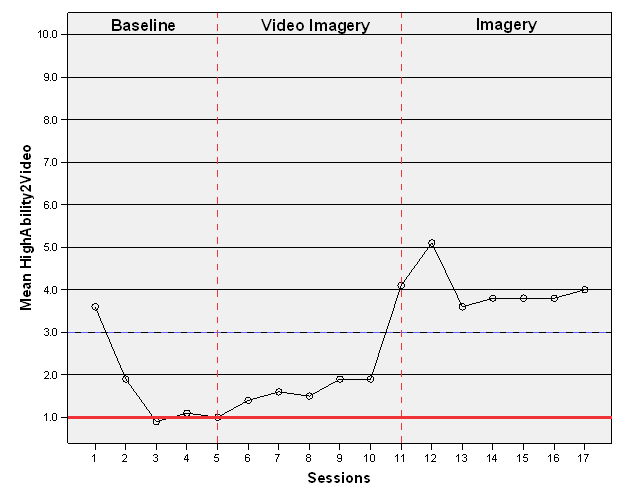
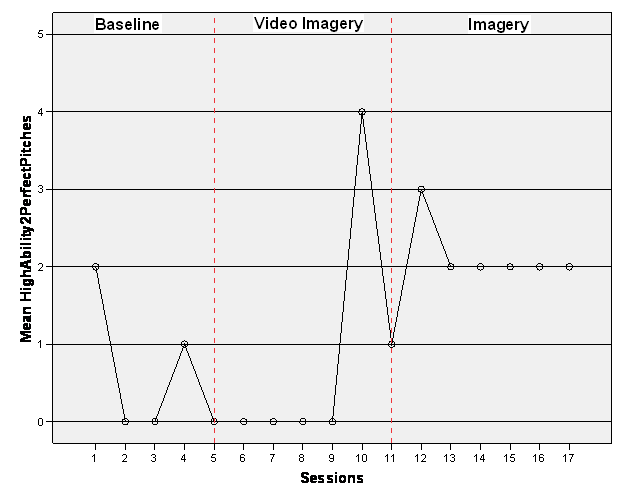
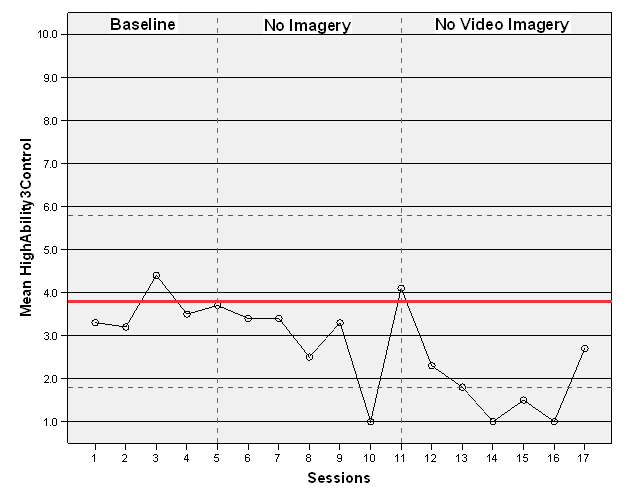
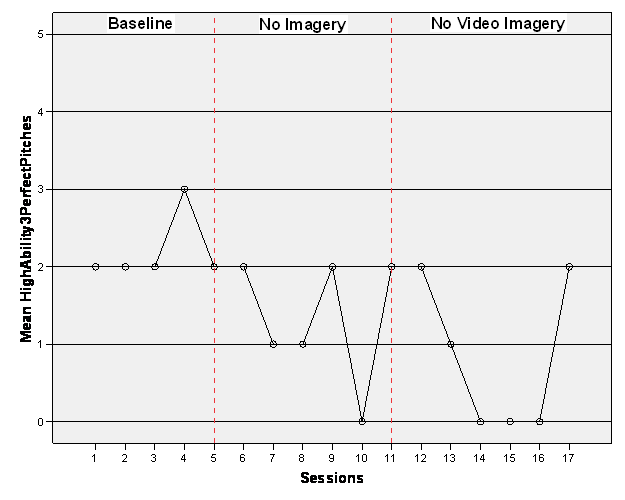
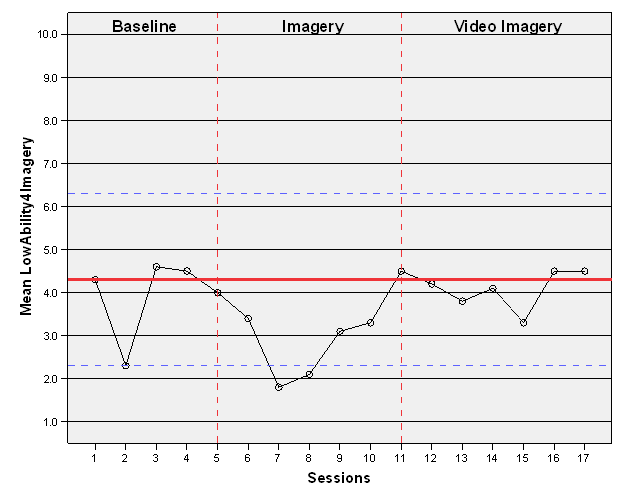
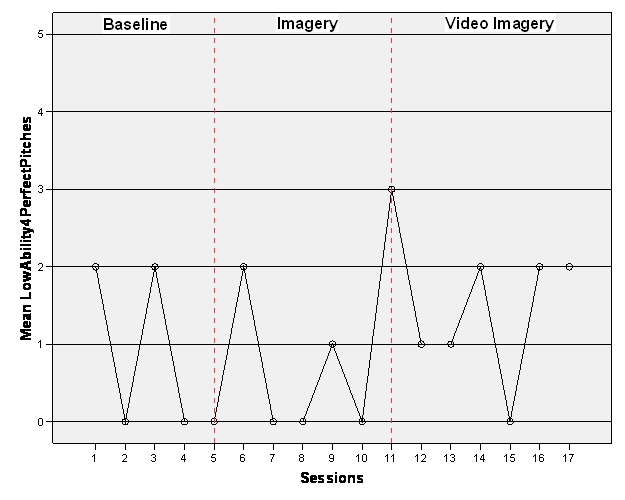
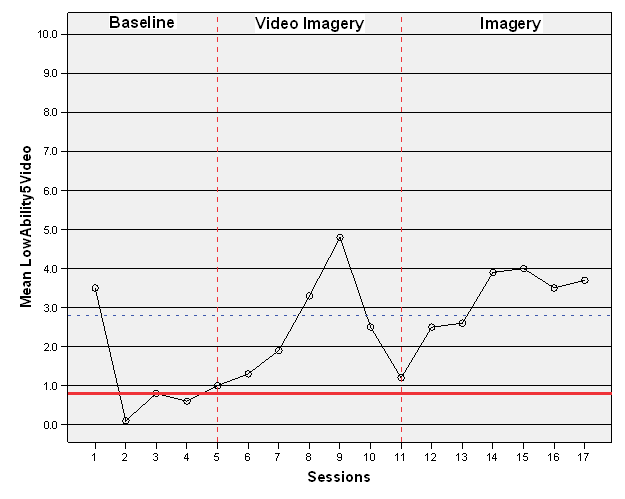
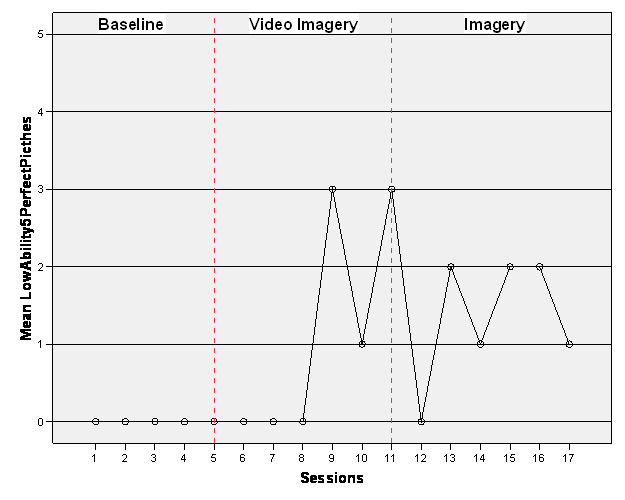
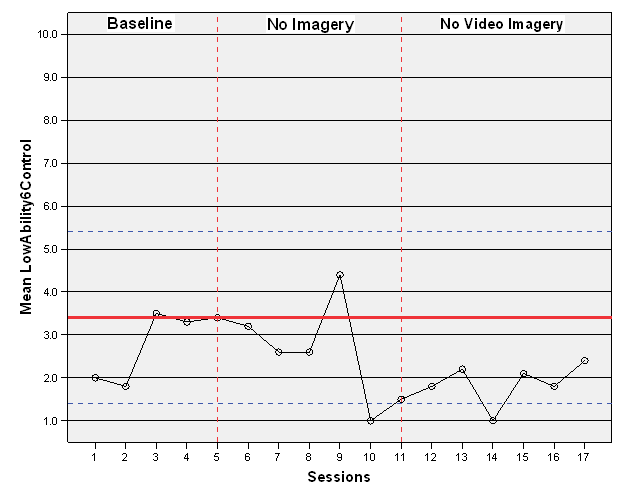
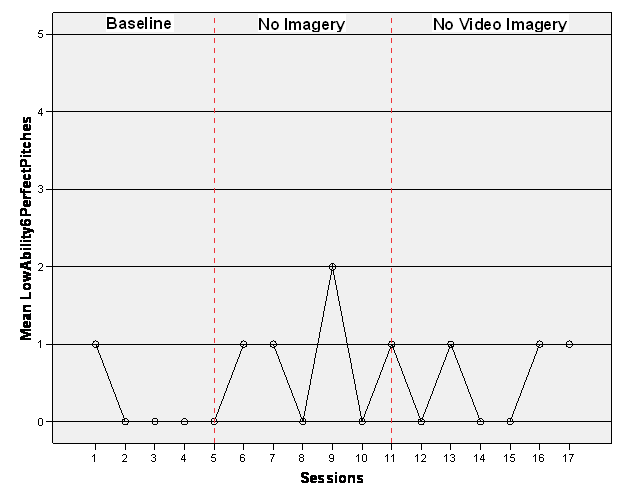
RESULTS Data collected for this study were evaluated using mixed methodological procedures from ocular statistics (Carboni, et al, 200); additionally, they are explored in qualitative terms. Figures 1–6 will illustrate the participants’ throwing performance scores over the length of the study. Figures 7–12 will illustrate perfect pitch count scores over the length of the study.
Table 1 presents the participants’ throwing performance scores, with standard deviations. Table 2 presents a count of perfect pitches thrown by the participants.
Table 1
Participants’ throwing accuracy scores*
Session
Number
High- Ability Participant
1
(C.I./ V.I.)
High- Ability Participant
2
(V.I./ C.I.)
High- Ability Participant
3
(Control)
Low- Ability Participant
4
(C.I./ V.I.)
Low- Ability Participant
5
(V. I./C.I.)
Low-
Ability Participant
6
(Control)
1
2.7 (3.2)
3.6 (4.7)
3.3 (4.0)
4.3 (3.8)
3.5 (3.7)
2.0 (3.1)
2
2.5 (3.0)
1.9 (3.0)
3.2 (4.0)
2.3 (2.6)
.1 (3.2)
1.8 (2.4)
3
3.4 (4.5)
.9 (1.9)
4.4 (3.7)
4.6 (4.2)
.8 (1.3)
3.5 (3.2)
4
2.5 (3.6)
1.1 (3.1)
3.5 (4.5)
4.5 (3.5)
.6 (1.9)
3.3 (2.9)
5
3.2 (3.9)
1.0 (1.9)
3.7 (3.6)
4.0 (3.4)
1.0 (1.3)
3.4 (3.1)
6
3.2 (3.9)
1.4 (2.3)
3.4 (4.0)
3.4 (3.9)
1.3 (2.5)
3.2 (3.9)
7
3.0 (2.4)
1.6 (1.9)
3.4 (3.7)
1.8 (2.4)
1.9 (3.0)
2.6 (3.9)
8
1.4 (1.8)
1.5 (2.0)
2.5 (3.5)
2.1 (2.0)
3.3 (4.7)
2.6 (3.0)
9
3.6 (3.9)
1.9 (2.2)
3.3 (4.0)
3.1 (3.1)
4.8 (4.6)
4.4 (3.4)
10
3.9 (4.6)
1.9 (3.1)
1.0 (1.9)
3.3 (3.9)
2.5 (4.0)
1.0 (1.9)
11
3.8 (4.1)
4.1 (5.1)
4.1 (3.9)
4.5 (4.7)
1.2 (3.2)
1.5 (3.1)
12
3.5 (3.7)
5.1 (4.1)
2.3 (4.1)
4.2 (3.4)
2.5 (4.0)
1.8 (2.6)
13
3.9 (3.8)
3.6 (4.1)
1.8 (3.1)
3.8 (3.3)
2.6 (3.9)
2.2 (3.7)
14
5.3 (3.7)
3.8 (3.7)
1.0 (1.9)
4.1 (3.80
3.9 (3.3)
1.0 (1.9)
15
3.3 (3.5)
3.8 (4.0)
1.5 (1.8)
3.3 (2.4)
4.0 (4.1)
2.1 (2.8)
16
3.8 (3.8)
3.8 (3.9)
1.0 (1.1)
4.5 (4.1)
3.5 (4.6)
1.8 (3.4)
17
3.6 (3.7)
4.0 (3.7)
2.7 (4.3)
4.5 (3.5)
3.7 (3.5)
2.4 (3.6)
* Standard deviations in parentheses.
Table 2
Perfect pitches thrown
Session
Number
High- Ability Participant 1
High- Ability Participant 2
High- Ability Participant
3
Low- Ability Participant
4
Low- Ability Participant 5
Low- Ability Participant 6
1
1
2
2
2
0
1
2
1
0
2
0
0
0
3
2
0
2
2
0
0
4
1
1
3
0
0
0
5
2
0
2
0
0
0
6
2
0
2
2
0
1
7
0
0
1
0
0
1
8
0
0
1
0
0
0
9
2
0
2
1
3
2
10
3
4
0
0
1
0
11
2
1
2
3
3
1
12
1
3
2
1
0
0
13
2
2
1
1
2
1
14
2
2
0
2
1
0
15
1
2
0
0
2
0
16
2
2
0
2
2
1
17
1
2
2
2
1
1
The participants provided qualitative reports concerning imagery effectiveness (with the exception of Participant 3 and Participant 6, the control group receiving no intervention).
Participant 1
Participant 1 initially received cognitive imagery intervention (Cognitive Imagery First). Participant 1 had demonstrated a 2.9 (SD= 4.5, 3.6, 3.9) throwing performance baseline during the first week of the study; with one exception, each of his throwing performance scores fell above that baseline, ranging from 3.2 (SD= 3.9) to 3.9 (SD= 4.6) (See Table 1). The exception occurred in Session 8, for which the participant’s accuracy score was 1.4 (SD= 1.8). While this score was below the participant’s baseline, it was not beyond the margins of implied change set, for this study, at .9 (See Figure 1).
Figure 1. Participant 1 (high-ability): Accuracy scores (imagery/ video Imagery)
As the participant completed subsequent video imagery interventions, the accuracy scores remained above the baseline, ranging between 3.5 (SD= 3.7) and 5.3 (SD=3.7); throwing performance scores in Session 14 reached 5.3 (SD= 3.7), exceeding the margins of implied change, set at 4.9. During the baseline portion of the study, Participant 1 recorded between 1 and 2 perfect pitches (See Table 2), a rate maintained throughout the study, except during the imagery intervention portion, Sessions 6 through 11. During the imagery intervention portion, this participant’s perfect pitch count ranged from 0 to 3 (see Figure 7).
Figure 7. Participant 1 (high-ability): Perfect pitches thrown Post Study Imagery Questionnaire
Participant 1, who said he had never used imagery prior to entering this study, reported that he used imagery while playing in a game during the period of the study. He stated, “I would like to continue using imagery and practice it more before games. I feel like it really helps when I start rushing.” Participant 1 further reported that breathing techniques included in the relaxation portion of the imagery script helped him manage momentum and refocus his effort. Participant 1 expressed the opinion that video imagery was relatively more helpful in bringing about desired outcomes, although he found it difficult to mentally re-create accompanying sensations during the video imagery sessions.
Participant 2
Participant 2 initially received video imagery intervention (Video Imagery First). Participant 2 had established a baseline score of 1.0 (SD= 1.9) within the first week of the study; his throwing performance scores increased slowly during the first intervention, ranging from 1.4 (SD= 2.3) to 4.1(SD= 5.1) (see Table 1). Each of Participant 2’s throwing performance scores fell above the baseline; during Session 11, his score exceeded the established margins of implied change (see Figure 2).
Figure 2. Participant 2 (high-ability): Accuracy scores (video imagery/ imagery)
During Session 12 through Session 17 (the imagery intervention), all of Participant 2’s scores remained above the implied margin of change, which was set at 3.0; his scores ranged from 4.0 (SD= 3.7) to 5.1 (SD= 4.1). While establishing a baseline score during Session 2 through Session 5, Participant 2 recorded from 0 to 1 perfect pitch per session (See Table 2). During the video imagery intervention, his perfect pitch count remained at 0 until Session 10, when he threw 4 perfect pitches; in Session 11, he threw 1 perfect pitch. During the imagery intervention, which was his final intervention, Participant 2 threw either 2 or 3 perfect pitches per session (see Figure 8).
Post Study Imagery Questionnaire
Participant 2 reported never having used imagery prior to the study, but said he is currently employing it during games because his pitching performance improved following the start of the study. He stated, “I haven’t walked anybody, it must be working. I started trying to see the ball go where I want it to before I throw the pitch, and it really seems to help.” Moreover, Participant 2 expressed a desire to continue using imagery, for its benefits both to his accuracy and his confidence.
Participant 3
Participant 3 did not participate in any intervention (No Interventions). He had established a baseline score of 3.8 (SD= 3.6) within the first week of the study. During Session 6 through Session 11, his throwing performance scores ranged from 1.0 (SD= 1.9) to 4.1 (SD= 3.9) (see Table 1). All of these scores fell below his baseline score, except the Session 11 score of 4.1 (SD= 3.9). During Session 10, the participant scored 1.0 (SD= 1.9), dropping below the margin of implied change, set at 1.8 (see Figure 3). Figure 3. Participant 3 (high-ability): Accuracy scores (control; no intervention)
Participant 3’s throwing performance scores in Sessions 12–17 ranged from 1.0 (SD= 1.9) to 2.7 (SD= 4.3), falling below his established baseline. During Session 13 through Session 16, this participant’s scores descended to the level of the margin of implied change. During the baseline portion of the study, Participant 3 threw either 2 or 3 perfect pitches per session. Across the remainder of the study, however (Sessions 6–17), Participant 3 threw 0, 1, or 2 perfect pitches per session (see Figure 9).
Participant 4
Participant 4 received cognitive imagery intervention first (Cognitive Imagery First). Participant 4 had established a baseline score of 4.3 (SD= 3.8) in the first week of the study, and during the first intervention, his throwing performance scores largely fell below that baseline, ranging from 1.8 (SD= 2.4) to 4.5 (SD= 4.7) (see Table 1). Session 11 comprised an exception.
Participant 4’s Session 11 score was 4.5 (SD= 4.7). During Session 7 and Session 8, the participant’s scores were 1.8 (SD= 2.4) and 2.1 (SD= 2.0), respectively, falling below the implied margin of change, which was set at 2.3. During Sessions 12–17, Participant 4 received video imagery intervention. His throwing performance scores for those sessions ranged from 3.3 (SD= 2.4) to 4.5 (SD= 3.5), and most fell below his baseline score, although his scores for Session 16 and Session 17 was 4.5 (SD= 4.1, 3.5) (see Figure 4).
During the baseline portion of the study, Participant 4 threw between 0 and 2 perfect pitches per session, a range he would go on to maintain for the duration of the study, excepting only Session 11, during which he threw 3 perfect pitches (see Figure 10).
Post Study Imagery Questionnaire
Participant 4 reported that he had used imagery prior to this study; he furthermore reported having difficulty sustaining the vividness of imagery. He went on to express a preference for having a detailed imagery script read to him, due to such reading’s capacity to generate vivid images. Participant 4 stated, “I usually do imagery before my games that I know I’m going to be pitching in. It helps me get focused, and I want to get better at it.” Participant 4 expressed a desire to continue imagery use, but made no note of any distinction between the cognitive and video approaches.
Participant 5
Participant 5 received video imagery intervention first (Video Imagery First). Participant 5 had established a baseline score of .8 (SD= 1.3) in the first week of the study. His throwing performance scores during the first intervention ranged from 1.2 (SD= 3.2) to 4.8 (SD= 4.6), above the baseline score he had produced (see Table 1). In Session 8 and Session 9, Participant 5 recorded scores of 3.3 (SD= 4.7) and 4.8 (SD= 4.6), respectively, exceeding the margin of implied change, which was set at 2.8 (see Figure 5). Figure 5. Participant 5 (low-ability): Accuracy scores (video imagery/ imagery)
During Session 12 through Session 17 (the imagery intervention portion of the study), Participant 5’s throwing performance scores ranged from 2.5 (SD= 4.0) to 4.0 (SD= 4.1). All scores thus fell above his baseline score, and his scores in Sessions 14–17 exceeded the margin of implied change, coming in between 3.5 (SD= 4.6) and 4.0 (SD= 4.1). During the baseline portion of the study, Participant 5 threw 0 perfect pitches. During Session 9 in the video imagery portion of the study, he threw 3 perfect pitches; in Session 10 he threw 1 perfect pitch; in Session 11 he again threw 3. Over Sessions 12–17, the participant threw anywhere from 0 to 2 perfect pitches (the 0 was recorded during Session 12; for each of the next 5 sessions, a 1 or 2 score was recorded; see Figure 11).
Post Study Imagery Questionnaire
Participant 5 reported never having used imagery prior to the study. He reported considering adherence to use of pre-game imagery following conclusion of the research project. Participant 5 reported noticing not only improved throwing accuracy, but increased self-confidence as well. He stated, “When I stop between each pitch, take a breath and see where I want the ball to go, it helps me to refocus. Also, when I do throw a bad pitch, it doesn’t carry over as much. I don’t get caught in a bad momentum. I am more able to release the last pitch and trust the next one, because I’ve seen myself throw it where I want to put the ball (in my head) many more times before. I know I can do it.”
Participant 6
Participant 6 belonged to the control group (No Intervention) and established a baseline score of 3.4 (SD= 3.1) during the study’s first week. His throwing performance scores ranged from 1.0 to 4.4 over Session 6 though Session 11 (see Table 1). With the exception of a 4.4 (SD= 3.4) throwing performance score in Session 9, Participant 6’s subsequent scores fell below his baseline score. During Session 10, Participant 6 recorded a throwing performance score of 1.0 (SD= 1.9), below the set 1.4 margin of implied change (see Figure 6).
Figure 6. Participant 6 (low-ability): Accuracy scores (control; no intervention)
Participant 6’s throwing performance scores for Sessions 12–17 were between 1.0 (SD=1.9) and 2.4 (SD= 3.6), all falling below the baseline. Moreover, in Session 14, the participant scored a 1.0 (SD= 1.9), which fell below the margin of implied change. While establishing his baseline score for this study, Participant 6 threw 0 perfect pitches. In Sessions 6–11, he threw from 0 to 2 (in Session 9) perfect pitches per session. For the remainder of the study (Sessions 12–17), he threw 0 to 1 perfect pitch per session (see Figure 12). Figure 12. Participant 6 (low-ability): Perfect pitches thrown
DISCUSSION
The purpose of the present study was to see whether imagery would have an effect on the throwing performance of individual baseball pitchers. Further, the present study sought to determine if individual variation in ability to “image” is associated with distinct responses to cognitive imagery interventions and video imagery interventions. By the end of Session 9, study Participants 1, 2, and 5 demonstrated higher scores (as compared to their individually established baseline scores) for throwing accuracy. This result parallels similar single subject sport-and-imagery research (Kearns & Crossman, 1992; Munroe-Chandler, Hall, Fishurne, Shannon, 2005; Shambrook & Bull, 1996; Templin & Vernacchia, 1993, 1995; Stewart, 1997, Carboni et al., 2000;). There should be further investigation into the effectiveness of brief interventions, because no research to date answers the old question of how frequent and how long intervention must be to produce the desired result (Cumming, Hall, Shambrook, 2007; Thelwell, Greenless, & Weston, 2006). The suggestion has been made that, as in the realm of physical skills, psychological-skills practice effects positive change only after an extensive investment of time (Weinberg & Williams, 2001). Thelwell, Greenless , and Weston (2006) found that combining three types of intervention—imagery, self-talk, and relaxation—produced results within a 3-day period, when 1 day of imagery training was provided and when measures were taken once weekly over a 9-match period. Murphy (1990) recommends intervention sessions of no more than 10 minutes’ duration, and Weinberg and Gould (2007) suggest providing intervention 3 to 5 times a week. Bull (1995) found that positive results ensued from a 4-week training period featuring 8 training sessions. Some researchers have examined intervention frequency and length by leaving participation to the discretion of the participant and recording objective reports; sessions as brief as 1 minute were noted (Carboni et al., 2000). Cumming, Hall, and Shambrook (2007) concluded that overall use of imagery could be increased with interventions as brief as a “workshop.” Findings from the present study indicate that, to be effective for specific tasks such as accurate pitching, imagery interventions can be as brief as 10 minutes in length, conducted 4 times weekly for 3 weeks.
The present study did not find participants to be affected distinctly by the two types of intervention (cognitive and video). The higher throwing performance score recorded for the final 6 sessions of the study are believed to reflect the lengthening period of time during which participants had practiced imagery practice, rather than to the type of intervention, since all participants receiving intervention responded similarly, whether they were in the Cognitive Imagery First group or Video Imagery First group. Gordon, Weinberg, and Jackson (1994) found similar results, investigating “internal” as opposed to “external” imagery. Future research into the effects of multiple interventions should seek to determine the relationship between effectiveness and time invested in each intervention.
Research has shown that imagery ability is a large determinant of how an individual’s physical performance will respond to imagery interventions (Hall, 1998). In the present study, however, scores for Participant 2 and Participant 5 (on both throwing accuracy and perfect pitches) improved more than they did among the other participants. That Participant 2 and Participant 5 succeeded more markedly with imagery use cannot, however, be attributable to higher-ability imagery, because Participant 2 was a high-ability imager while Participant 5 was a low-ability imager. Any individual, regardless of imagery ability, can benefit from imagery practice, although those with lower ability may continue to experience greater difficulty creating and controlling vivid imagery (Magill, 2007). Each high school level participant from the present study had a baseline score for throwing accuracy that was lower than the lowest such score established by a college level participant. Isaac and Marks (1994) and Piaget and Inhelder (1971) concur that imagery ability is developed by age 7. Moreover, Payne and Isaacs (1995) report that the highest level of cognition and abstract thinking develops at age 11–12. Participants 2 and 5 had a mean age of 17, beyond the developmental period and ranking them developmentally equal to the college level participants. The distinct intervention responses of Participants 2 and 5, then, are not due to the basic development of ability to image. Research on imagery use has found differences associated with subjects’ athletic competitive levels (Barr & Hall,1992; Salmon, Hall, & Haslam, 1994; Vadocz et al., 1997). These differences seem to be shaped by factors like years of experience, degree of motivation to play, degree of motivation to use imagery, and ability to create and control images.
Thelwell, Greenless, and Weston (2006) discuss ways in which distinct levels of goal orientation affect players’ levels of investment in imagery use. Research also finds that athletes exhibiting moderate to high levels of task and ego orientation become more invested in imagery use, in turn increasing how often they practice imagery (Cumming, Hall, Gammage, & Harwook, 2002; Harwood, Cumming, & Hall, 2003). Bull (1995) examined the effects of a 4-week mental training program on varsity athletes, finding that better-motivated athletes were likelier to adhere to an imagery program, and that less-seasoned athletes were likelier to be the better motivated. It is possible that Participants 2 and 5 in our study, being at one of the earliest stages of an athletic career, were better motivated than Participants 1, 3, and 4, who were playing what they anticipated would be the final season of their careers.
Motivation can also be affected by fatigue and overtraining. The participants in the present study all were at mid-season, obligated to a vigorous training schedule as well as to the study sessions. At least one point during the study, every participant reported feeling fatigue or exhaustion, and this might have affected their concentration and performance. A perceived imbalance between demands on athletes and their response capabilities sometimes creates the negative physical and emotional state known as burnout (Creswell & Eklund, 2006). As Creswell and Eklund (2006) state, insufficient “rest and recovery periods” will also help generate negative experiences. Participants in the present study might possibly have found that study-related testing and intervention consumed the time they normally would use for recovery and rest, which could account, to some degree, for periodic “off” performance, including uncharacteristically low accuracy scores, trending down of accuracy scores, loss of interest in the study, or transfer of effort from the study to some other task. The performance of Participant 3 and Participant 6 support such an interpretation; these two athletes received no intervention and saw their performance fall off over time. “Burnout” may also help describe the expressed attitudes of Participants 1, 3, 4, and 6.
The study’s timing during the athletes’ season may help explain any shortages of focus or concentration on their part, but additional distractions should also be considered. During video imagery intervention sessions, for example, certain participants showed clear difficulty in focusing when they opened their eyes at the conclusion of the relaxation portion in order to view video. The discrepancy arose even though all of the imagery sessions took place in the university’s Mental Edge Training Facility, where each participant was assured of experiencing interventions of identical length. To better maintain focus and a relaxed state, future research might employ a different viewing method (e.g., use a dark room into which video is introduced from outside or use virtual-reality gear). Furthermore, researchers would be well advised to employ a vivid script that helps participants to incorporate as many types of sensation as possible (Thelwell, Greenless, & Weston, 2006). The script used in the present study instructed participants to “see” only the target’s center box, which perhaps explains in part why Participant 2 and Participant 5 were able to throw more perfect pitches (see Figure 8 and Figure 11).
For the present study, throwing performance was defined as a pitcher’s ability to throw a ball at a specified area deemed the target. In measuring throwing performance, the mean score for the 10 pitching efforts made each session was recorded and graphically represented. Perfect pitches were defined as those hitting the center target, and they too were recorded and graphically represented; a perfect pitch received a score of 10 points.
There are various definitions of what performance enhancement actually is. Some individuals may look for greater consistency, more pitches thrown closer to target, when seeking evidence of performance enhancement. Others may see enhanced performance in a combination of more pitches thrown at the actual target, and lower-scoring pitches. For the present study, the mean score and number of perfect pitches thrown for each session were used to measure performance response. During cognitive imagery interventions, participants were asked to envision throwing only to the center box, while during video imagery interventions, they watched tapings of pitches thrown to the center box. An increase in pitches to the center box was, for this reason, said to indicate imagery intervention’s positive effects on throwing performance.
Two limitations on the present study resulted from the data collection process. First, during the intervention sessions, participants were exposed to extraneous noise, although none directly identified this as a distraction. In future studies, areas free of extraneous noise should be employed. Second, when a participant was unable to join in throwing performance measurement or imagery intervention session during daylight hours, the researchers accommodated his schedules by conducting these activities after dark, an inconsistency which, by potentially affecting vision, perhaps also affected success. Furthermore, time of day bears on the level of concentration and fatigue.
Results obtained through the Post Study Imagery Questionnaire describe perceived positive effects imagery wields on athlete performance and confidence. This questionnaire also documents that participants’ appreciation for psychological skills training grew during the study. These findings parallel past research (Carboni et al., 2000; Kearns & Crossman, 1992; Shambrook & Bull, 1996; Templin & Vernacchia, 1993, 1995; Stewart, 1997; Thelwell et al., 2006). Participants 1, 2, and 5 expressed an outlook positive toward the imagery sessions, toward their own confidence concerning tasks, and toward anxiety-reducing effects of mentally re-creating a pitching sequence. This supports numerous findings about imagery’s possible benefits, for example improved self-confidence (Callow, Hardy, & Hall, 2001), better motivation (Callow & Hardy, 2001), improved regulation of arousal (Hecker & Kaczor, 1988), and stronger ability to modify such cognitions as self-efficacy (Feltz & Ressinger, 1990). Imagery, or mental practice, can, the research record demonstrates, be used to control anxiety and to enhance both the strategies and physical movements that will be employed in performing a skill (Magill, 2007).
Suggestions for future research include, again, the deployment of alternative methods of presenting video imagery intervention, to ensure participants’ focus is maintained. In addition, future research should examine how often and for how long interventions are best administered, in terms of performance enhancement.
The baselines established by this study’s participants did not vary more than 1 point, although the criterion we employed for defining baseline and actual change was 2 points (on a 10-point scale). Perhaps future research would benefit from more strict criteria, which would tend to identify more pronounced effects.
Psychological skills training, coaches and athletes often fear, entails a long-term commitment and many field practice hours lost. The present findings, however, imply that imagery training’s effects on at least the one position-specific task studied are observable in as little as twelve 10-minute sessions (4 per week for 3 weeks). Moreover, the study demonstrates that effective intervention may take place during the competetive season and in conjunction with rigorous physical training.
Bull (1991) identified three barriers between athletes and ongoing psychological skills training: time constraints, a disruptive home environment, and an unmet need for individually tailored training. The position-specific intervention employed in this study, together with use of a brief script, alleviate all three problems. Later, in a discussion of how best to implement psychological skills training, Shambrook and Bull (1999) emphasized the importance of time management, of structure, and of integration of psychological skills within existing training. The present study’s findings, past research focusing on workshops (Cummings, Hall, & Shambrook, 2007), and future research will complete the path around the barriers, driving home that intervention programs may be both brief and integrated within established physical training in order to reap positive returns.
REFERENCES
Albinson, J. G., & Bull, S. J. (1988). The mental game plan. London, Ontario, Canada: Spodym.
Betts, G. H. (1909). The distributions and functions of mental imagery. New York: Teachers College Columbia University.
Bryan, A. J. (1987). Single-subject designs for evaluation of sport psychology interventions. The Sport Psychologist,1, 283–292.
Bull, S. J. (1991). Personal and situational influences on adherence to mental skills training. Journal of Sport and Exercise Psychology, 13, 121–132.
Callow, N., & Hardy, L. (2001). Types of imagery associated with sport confidence in netball players of varying skill levels. Journal of Applied Sport Psychology, 13, 1–17.
Callow, N., Hardy, L., & Hall, C. (2001). The effects of a motivational general-mastery imagery intervention on the sport confidence of high-level badminton players. Research Quarterly for Exercise and Sport, 72, 389–400.
Camels, C., Holmes, P., Berthoumeius, C., Paris, F., & Singer, R. (2004). The development of movement imagery vividness through a structured intervention in softball. Journal of Sport Behavior, 27, 307–322.
Carboni, J., Burke, K., Joyner, A. B., Hardy, C. J., & Blom, L. C. (2000). The effects of brief imagery on free throw shooting performance and concentration style of intercollegiate basketball players: A single subject design. International Sports Journal, 6, 60–68.
Carpenter, W. B. (1894). Principles of mental physiology. New York: Appleton.
Corbin, C. B. (1972). Mental practice. In W. P. Morgan (Ed.), Ergogenic Aids and Muscular Performance (pp 93-118). New York: Academic.
Creswell, S. & Eklund, R. (2007). The nature of player burnout in rugby: Key characteristics and attributions. Journal of Applied Sport Psychology, 18, 219, 232
Cumming, J., & Hall, C. (2002a). Deliberate imagery practice: Examining the development of imagery skills in competitive athletes. Journal of Sport Sciences, 20, 137–145.
Cumming, J., & Hall, C. (2002b). Athletes’ use of imagery in the off-season. The Sport Psychologist, 16, 160–172.
Cumming, J., Hall, C., Harwood, C. G., & Gammage, K. (2002). Motivational orientations and imagery use: A goal profiling analysis. Journal of Sport Sciences, 20, 127–136.
Cumming, J., Hall, C., & Shambrook, C. (2007). The influence of an imagery workshop on athletes’ use of imagery. Athletic Insight: Online Journal of Sport Psychology,6, 1.
Driskell, J. E., Copper, C., & Moran, A. (1994). Does mental practice enhance performance? A meta-analysis. Journal of Applied Psychology, 79, 481–492.
Feltz, D. L., & Riessinger, C. A. (1990). Effects of in vivo imagery and performance feedback on self-efficacy and muscular endurance. Journal of Sport and Exercise Psychology, 12, 132–143.
Gordon, S., Jackson, A., & Weinberg, R. (1994). Effect of internal imagery on cricket performance. Journal of Sport Behavior, 17.
Goss, S., Hall, C. R., Buckolz, E., & Fishbourne, G. J. (1986). Imagery ability and the acquisition and retention of movements. Memory and Cognition, 14, 469–477.
Gould, D., Dieffenbach, K., & Moffett, A. (2002). Psychological characteristics and their development in Olympic champions. Journal of Applied Sport Psychology, 14, 172–204.
Gould, D., Petlichkoff, L., Hodge, K., & Simons, J. (1990). Evaluating the effectiveness of a psychological skills educational workshop. The Sport Psychologist, 4, 249–260.
Hale, B. D. (1982). The effects of internal and external imagery on muscular and ocular concomitants. Journal of Sport Psychology, 4, 379–387.
Hall, C. (1998). Measuring imagery abilities and imagery use. In J. Duda (Ed.), Advances in sport and exercise psychology measurement (pp. 165–172). Morgantown, WV: Fitness Information Technology.
Hall, C. (2001). Imagery in sport and exercise. In R. Singer, H. Hausenblas, & C. Janelle (Eds.), Handbook of Sport Psychology (pp. 529–549). New York: John Wiley & Sons.
Hall, E. G., & Erffmeyer, E. S. (1983). The effect of visuo-motor behavior rehearsal with videotaped modeling on free throw accuracy of intercollegiate female basketball players. Journal of Sport Psychology, 5, 343–346.
Hall, C. R., Pongrac, J., & Buckholz, E. (1985). The measurement of imagery ability. Human Movement Science, 4, 107–118.
Hall, C. R., & Pongrac, J. (1983). Movement imagery questionnaire. London, Ontario, Canada: University of Western Ontario, Faculty of Physical Education.
Hecker, J. E., & Kaczor, L. M. (1988). Application of imagery theory to sport psychology: Some preliminary findings. Journal of Sport and Exercise Psychology, 10, 363–373.
Isaac, A. R., & Marks, D. F. (1994). Individual differences in mental imagery experience: Developmental changes and specialization. British Journal of Psychology, 85, 479–500.
Kearns, D. W., & Crossman, J. (1992). Effects of a cognitive intervention package on the free-throw performance of varsity basketball players during practice and competition. Perceptual and Motor Skills, 75, 1243–1253.
Magill, R.A. (2007). Motor learning and control: Concepts and applications. New York: McGraw-Hill
Moritz, S. E., Hall, C., Martin, K. A., & Vadocz, E. (1996). What are confident athletes imaging? An examination of image content. The Sport Psychologist, 10, 171–179.
Munroe, K. J., Giacobbi, P. R., Hall, C., & Weinberg, R. (2000). The four Ws of imagery use: Where, when, why, and what. The Sport Psychologist, 14, 119–137.
Murphy. S., Jowdy, D., & Durtschi, S. (1990). Report on the U. S. Olympic Committee survey on imagery use in sport. In R. Weinberg & D. Gould (Eds.), Foundations of Sport & Exercise Psychology (p. 293). Champaign, IL: Human Kinetics.
Orlick, T. (1990). In pursuit of excellence: How to win in sport and life through mental training. Champaign, IL: Human Kinetics.
Paivio, A. (1985). Cognitive and motivational functions of imagery in human performance. Canadian Journal of Applied Sports Sciences, 10, 22S–28S.
Payne, V. G., & Isaacs, L. D. (1995). Human motor development: A lifespan approach (3rd ed.). Mountain View, CA: Mayfield.
Piaget, J., & Inhelder, B. (1971). Mental imagery in the child. New York: Basic Books.
Salmon, J., Hall, C., & Haslam, I. (1994). The use of imagery by soccer players. Journal of Applied Sport Psychology, 6(1), 116–133.
Shambrook, C. J., & Bull, S. J. (1996). The use of a single-case research design to investigate the efficacy of imagery training. Journal of Applied Sport Psychology, 8, 27–43.
Shambrook, C., & Bull, (1999). Adherence to psychological preparation in sport. In S. J. Bull (Ed.), Adherence issues in sport and exercise (pp. 169–196). New York: John Wiley & Sons.
Shiffman, H. R. (1995). The skin, body and chemical senses. In R. L. Gregory & A. M. Colman (Eds.), Sensation and Perception (pp. 70–96). London: Longman.
Stewart, G. R. (1997). A single subject design to study the effects of a mental imagery intervention on basketball free-throw performance. Tesis de Master: Queen’s University
Stroksahl, K., & Ascough, J. C. (1981). A multiple component of clinical imagery. In E. Klinger (Ed.), Imagery: Concepts, results and applications (pp. 259–274). New York: Plenum.
Templin, D. P., & Vernacchia, R. A. (1995). The effect of highlight music videotapes upon the game performance of intercollegiate basketball players. The Sport Psychologist, 9, 41–50.
Thelwell, R., Greenless, I., & Weston, N. (2007). Using psychological skills training to develop soccer performance. Journal of Applied Sport Psychology,18, 254.
Vadocz, E., Hall, C., & Moritz, S. (1997). The relationship between competitive anxiety and imagery use. Journal of Applied Sport Psychology, 9, 241–253.
Vealey, R. S., & Walter, S. M. (1993). Imagery training for performance enhancement and personal development. In J. M. Williams (Ed.), Applied sport psychology: Personal growth to peak performance (pp. 200–223). Mountain View, CA: Mayfield.
Vealey, R. S., & Greenleaf, C. A. (2001). Seeing is believing: Understanding and using imagery in sport. In J. M. Williams (Ed.), Applied sport psychology: Personal growth to peak performance (4th ed.). Mountain View, CA: Mayfield.
Weinberg, R. S., & Williams, J. M. (2001). Integrating and implementing a psychological skills training program. In J. M. Williams (Ed.), Applied sport psychology: Personal growth to peak performance (4th ed.), pp. 347–377). Mountain View, CA: Mayfield.