Submitted by James N. Druckman, Northwestern University; Mauro Gilli, Northwestern University; Samara Klar, University of Arizona; Joshua Robison, Northwestern University.
Abstract:
Purpose: Few policies have been deemed as successful as Title IX, which, in theory, ensures equal educational opportunities for women. While the language of the law makes no mention of athletics, Title IX has nonetheless become a cornerstone of equality in athletics and the basis of expansion of sports programs for female athletes. As with any public policy, however, there is much debate about the ramifications, potential, and implementation of Title IX. Additionally, change and interpretation can be traced back, to a large extent, to public support or opposition. Yet, virtually no work explores public opinion about Title IX, particularly among the very issue public most affected by the law: college athletes.
Methods: A wide-scale survey of opinion and knowledge of Title IX among college athletes.
Results: The key correlates explaining support for Title IX are identified. A key finding is that nearly half of college respondents do not fully grasp the breadth of Title IX, which potentially limits the impact of the law.
Conclusions: Much educational efforts are needed concerning Title IX.
Application in Sport: The results show what characteristics shape support for Title IX, thereby providing guidance to individuals interested in promoting (or arguing against) the law. Perhaps most importantly, many affected student-athletes do not fully understand Title IX and thus educational efforts continue to be needed.
Submitted by Mark DeBeliso, Joe Walsh, Mike Climstein, Ian Timothy Heazlewood, Jyrki Kettunen, Trish Sevene and Kent Adams
ABSTRACT
Athletes competing at the World Masters Games have either initiated exercise later in life or pursued a physically active lifestyle for an extended period. There is a paucity of information regarding the prevalence of chronic health disorders for this unique cohort of mature adults. PURPOSE: To investigate the different aspects of health of the Sydney 2009 World Masters Games North American participants. METHODS: An online survey was developed to investigate participant demographics, physiological measures of health, and medical health history. Questionnaire responses were collected from competitors representing 95 countries in 28 sports. Data were culled to focus on North American participants for comparison purposes (Centers for Disease Control and Prevention). RESULTS: A total of 928 participants from Canada and the United States (age 52.6±9.8 yrs) completed the survey, with 55% reported having previously competed in the World Masters Games. The top five sports were football (25.6%), track and field (15.4%), swimming (8.4%), volleyball (8.2%), and softball (7.8%). Very few (2.5%) reported currently smoking with an average of 65 cigarettes per week, while 13.6% were ex-smokers. Alcohol consumption (82.0% of the participants) averaged 4.7 drinks week, while 0.6% were ex-drinkers. The top five chronic disorders were rheumatoid arthritis or osteoarthritis (10.0%), hypertension (HTN 9.1%), hyperlipidemia (8.0%), asthma (6.5%), and depression (5.3%). Top three operative treatments were knee replacement or repair (12.2%), hernia repair (6.1%), and herniated disc surgery (2.0%). Top four prescription medications were anti-HTN (6.9%), thyroid hormones (6.6%), hypolipidaemic (6.0%), and medications to increase bone strength (5.9%). Prevalence was significantly lower versus the general US population for HTN, hyperlipidemia, arthritis, asthma, and depression (all p-values <0.01). CONCLUSION: Chronic disease and disorder indicators reported by participants of the 2009 World Masters Games were significantly lower versus the general US population. APPLICATIONS IN SPORT: Competitive sport in mature aged participants requires adherence with physical activity. Exercise adherence in competitive masters sport may promote successful aging and a counter measure to many chronic diseases. (more…)
Submitted by Brandon Spradley, Sutthanuch Wiriyanpinit and Amber Magner
ABSTRACT Purpose: Athletic trainers and sport medicine professionals have the responsibility of diagnosing and managing concussion in athletes. The King-Devick (K-D) Test provides athletic trainers and sport medicine professionals with an easy-to-use concussion screening tool that requires only two minutes to administer and has relevance to contact sports such as football, soccer, boxing, and mixed martial arts. The purpose of this pilot study was to examine the reliability of baseline testing with the K-D Test in different environments.
Methods: A total of nine participants (6 males, 3 females, mean age: 39 ± 14.49 yrs) participated in the three day investigation. Subjects reported to the human performance laboratory on three separate days. Participants were given standard instructions for the K-D Test. Participants were required to complete the K-D test under a quiet environment (with minimal to no noise) and under two loud (noisy) environments; one with speakers and the other with headphones.
Results: Results indicated K-D scores for baseline (BL) and speakers (SP) rendered group means of (BL: 40.54 ± 14.95 s, SP: 40.54 ± 15.92 s), while scores for HP signified slightly lower group means of 39.54 ± 14.39 s. No variables showed any statistical difference in K-D scores (P > 0.05).
Conclusion: Most participants were able to improve their K-D scores from Trial 1 (T1) to Trial 2 (T2) on baseline testing, signifying a slight learning effect within the study group.
Application to Sport: Athletic trainers, healthcare professionals, and those administering the K-D Test should be consistent in assessing pre and post K-D scores, although significant changes might not occur when performing the K-D Test under different environments (with crowd noise). Athletes should be treated on an individual basis when using the K-D Test to assess pre and post test scores. (more…)
Submitted by Shelley L. Holden, Steven F. Pugh, Phillip M. Norrell and Christopher M. Keshock
Abstract
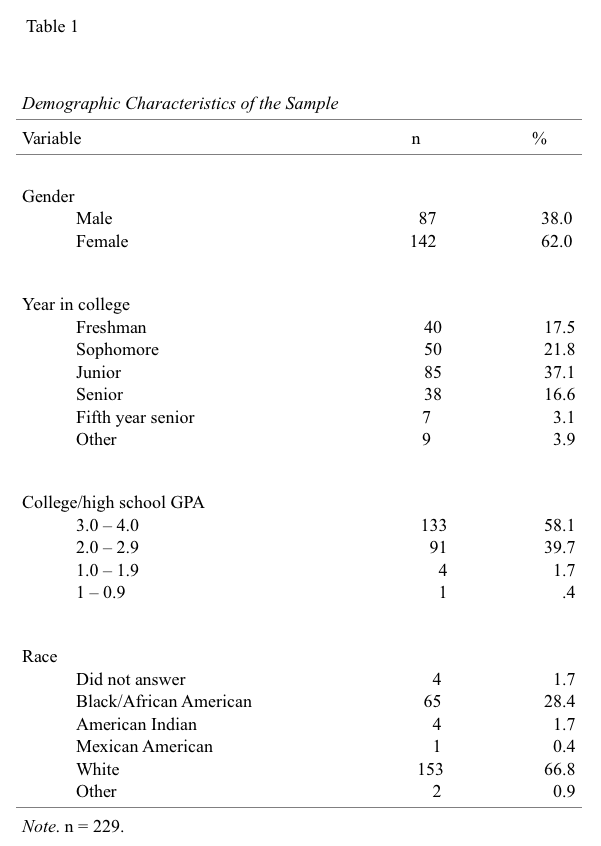
Alabama has one of the highest rates of obesity in the U.S. and nutritional knowledge may be a factor in those statistics. Recent studies found more than a third of U.S. adults, and over 16% of the population were obese in 2009-2010. In 1986, Alabama’s obesity rate was less than 10%, compared to more than 30% in 2010. The reasons cited for the increase included lack of nutritional knowledge. The purpose of this study was to determine the nutritional knowledge of undergraduate college students at one university in Alabama. The 229 participants (87 male, 142 female) were undergraduates enrolled in health and physical education courses at a state university. None previously had a college nutrition course. Ages ranged from 18 to 58 (M= 22.3). There were 40 freshman, 50 sophomores, 85 juniors, 38 seniors, 7 fifth year seniors, and 9 non-degree students. Nutritional knowledge was assessed using the Nutrition Knowledge Questionnaire (NKQ). The NKQ meets psychometric criteria for reliability (Cronbach’s alpha=.70-.97 and construct validity, P=.001). The NKQ is divided into subscales: Dietary Recommendations (DR), Sources of Foods (SOF), Choosing Everyday Foods (CEF), Diet-Disease Relationships (DDR), and Total Score (TS). The survey was administered the first day of class. Results indicated a lack of nutritional knowledge in all subscales of the NKQ. The mean scores were 6.98 (63.4%) on the DR, 35.3 (51.1%) SOF, 4.1 (41%) CEF, 5.1 (25.5%) DDR and 51.5 (46.8%) TS. Nutritional knowledge has been cited as a factor in increasing rates of obesity and by falling far short of an acceptable level on all the subscales the participants scores are a serious concern. Students lacked the nutritional knowledge to make good dietary choices. The researchers realize that other factors (genetics, physiology, exercise) play a role in obesity. However, students must be better educated in nutrition. Further, nutritional education guidelines as set by the State Course of Study need to be examined.
INTRODUCTION
It is estimated that 300,000 people in the United States die each year as a result of conditions relating to obesity and more than 60% of adolescents and adults are underactive (2). Obesity is a also a major concern in the United States due to rate at which it is increasing in the general population. In 2000, no state had a prevalence of obesity less than 10%, 23 states had between 20-24%, and none had rates of obesity greater than 25% (1). However, in 2010 no state had a prevalence of obesity less than 20%, 36 states had a prevalence equal to or greater than 25% and 12 of these states (Alabama, Arkansas, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Oklahoma, South Carolina, Tennessee, Texas and West Virginia) had a prevalence equal to or greater than 30% (1, 2). Further, more than one third of adults and approximately 17% of U. S. youth were considered obese in 2009-2010 (5).
This is of great concern because of the rising costs of healthcare associated with the chronic diseases related to obesity. On average obesity costs the U. S. health care system $117 billion per year in direct medical costs, but does not include indirect expenses (loss of wages and decreased productivity) (2).
Alabama has not been immune to the increase in its obese population. In 1986, Alabama had an obesity rate of less than 10% compared to more than 30% in 2010 (1-3). Other concerns are the variables involved in the increase in rate of obesity within the state. Prior research has indicated the lack of nutritional knowledge as a potential variable in the increase in the prevalence of obesity within the state. Therefore, the purpose of the current study was to determine the nutritional knowledge of Alabama undergraduate college students with no prior nutrition course at the college level.
Methods
Participants
The 229 participants (87 male, 142 female) in this study were undergraduates enrolled in health and physical education courses at a state university. None of the participants in the study had previously taken a college nutrition course.
Measures
For the purposes of this study, the following definition of obesity was used: Obesity: body mass index (BMI) > 30. BMI is calculated as weight in kilograms divided by height in meters squared, rounded to one decimal place (4).
Nutritional knowledge was assessed using the Nutrition Knowledge Questionnaire (NKQ) that was developed by Parmenter and Wardle (6). The NKQ meets psychometric criteria for reliability (Cronbach’s alpha=.70-.97 and construct validity, P=.001). Validity and reliability studies have been conducted on the questionnaire as a whole, as well as, each section separately (6).
The NKQ is divided into four independent sections and a total score: Dietary Recommendations (DR), Sources of Foods/Nutrients (SOFN), Choosing Everyday Foods (CEF), Diet-Disease Relationships (DDR), and Total Score (TS). Each correct answer in the section carried a point value of one and each section also had a corresponding maximum score (Section I- DR= 11, Section II- SOFN= 69, Section III- CEF= 10, Section IV- DDR= 20 and TS= 110).
Procedures
Approval for the study was obtained from the Institutional Review Board (IRB) of the researcher’s university. The survey was administered the first day of class before any type of nutrition lesson was taught. The researcher eliminated all surveys of participants who had previously taken a nutrition course at the college level (junior college or 4-year college), those who were graduate students, and those who did not complete all questions on the instrument. Therefore, 116 participants were omitted from this study.
The dependent variables in this study were the sections of the NKQ (Dietary Recommendations (DR), Sources of Foods/Nutrients (SOFN), Choosing Everyday Foods (CEF), Diet-Disease Relationships (DDR), and Total Score (TS). The independent variable was undergraduate students enrolled in the health and physical education courses offered at the university.
Results
Table 1 presents the demographic characteristics of the sample. Ages of the participants ranged from 18 to 58 (M= 22.3). Thirty-four (14.8%) of the participants were on an intercollegiate athletics team at the university and 195 (85.2%) were not. In terms of nutritional knowledge, results indicated a lack of nutritional knowledge in all sections of the NKQ. The mean score was 6.98 (63.4%) on the DR section which measures Dietary Recommendations. That is, an indication that the participants had little knowledge of the categories of food selections, the recommended servings for those categories, or what is considered a portion amongst the various categories. The mean score was 35.3 (51.1%) in the SOF section which measures sources of nutrients in foods. The mean score was 4.1 (41%) in the CEF section which measures choosing everyday foods which includes the ability to make healthy and unhealthy choices. The mean score was 5.1 (25.5%) in the DDR section that measures the diet-disease relationship. More specifically, foods that are related to health issues such as limiting saturated fats. Finally, the mean total score on the instrument was 51.5 (46.8%) which is a measure of overall knowledge.
Conclusions
Nutritional knowledge has been cited as a factor in increasing rates of obesity and the results of the current study support this factor. Moreover, the undergraduates’ scores falling far short on all the sections could indicate a general lack of nutritional knowledge and therefore, a serious concern with regard to the rising rates of obesity in the state. Students in the current study lacked the nutritional knowledge to make sound dietary choices. The researchers realize that factors other than nutritional knowledge such as genetics, physiology, mindfulness and exercise play a role in obesity too, but the lack of nutritional knowledge of the students in this study cannot be ignored.
Nutritional education guidelines as set by the State Course of Study in elementary, middle, and high school need to be examined to ensure adequate coverage of this vital topic if the rate of obesity is to be halted or preferably lowered. Also, it is imperative that teachers instructing health courses actually follow and meet the standards set forth in the courses of study. Adequate preparation of teachers is also an issue as noted by Graves, Farthing, Smith, and Turchi, (3) and Scofield and Unruh (7). “Sport coaches” who often have a lack of sufficient nutritional knowledge tend to teach health and nutrition courses and/or provide student athletes with nutritional information that could be potentially incorrect or insufficient. This is of grave concern because research has cited high school coaches as one of the most likely sources for students to seek nutritional knowledge (7, 2).
Applications in Sport
It is vital that we ensure that the information provided to students regarding nutrition is accurate and that there is an identifiable source for this information in the course of study.
Future research might examine the degree to which nutrition is covered in the state courses of study, and the degree to which the standards in the course of study are met within the K-12 classes. Another interesting inquiry would be to use body composition rather than Body Mass Index (BMI) as a measure of obesity as body composition, not BMI, is the major health concern. Body Mass Index, particularly in athletes, may show a false positive reading for overweight as many athletes’ musculature would indicate them as overweight using BMI when their body fat might be well within a health range.
ACKNOWLEDGMENTS
None
REFERENCES
1. Center for Disease Control. (2012). Obesity trends among U.S. adults between 1985-2010. Atlanta, GA: Author.
2. Edwards, B. (2005). Childhood obesity: a school-based approach to increase nutritional knowledge and activity levels. Nursing Clinics of North America, 40, 661-669. doi:10.1016/j.cnur.2005.07.006
3. Graves, K. L., Farthing, M. C., Smith, S. A, & Turchi, J. M. (1991). Nutritional training, attitudes, knowledge, recommendations, responsibility, and resource utilization of high school coaches and trainers. Journal of the American Dietetic Association, 91(3), 321-324.
4. National Center for Health Statistics. (2010, December). Obesity and socioeconomic status in adults: United States, 2005-2008 (Issue Brief No. 50). Hyattsville, MD: Ogden, C.L., Lamb, M. M., Carroll, & Flegal, K. M.
5. National Center for Health Statistics. (2012, January). Prevalence of obesity in the United States, 2009-2010 (Issue Brief No. 82). Hyattsville, MD: Ogden, C.L., Carroll, M. D., Kit, B. K., & Flegal, K. M.
6. Parmenter, K. & Wardle, J. (1999). Development of a general knowledge questionnaire for adults. European Journal of Clinical Nutrition, 53, 298- 308.
7. Scofield, D. E., Unruh, S. (2006). Dietary supplement use among high school athletes in central Nebraska and their sources of information. Journal of Strength and Conditioning Research, 20(2), 452-455. Doi:10.1519/R- 16984.1.
Submitted by Gillian Hotz Ph.D, Ashlee Quintero, BSc, Ray Crittenden, MSc, Lauren Baker, David Goldstein and Kester Nedd, DO
ABSTRACT Background: With the national spotlight on concussions sustained in contact sports, this Countywide Concussion Program addresses the unique challenges presented to public and private high schools in order to increase concussion awareness, identification, and management.
Methods: The Miami Concussion Model (MCM) was developed with a standard protocol that includes; formation of a task force of stakeholders, concussion education and training to coaches, athletic trainers, and athletes; baseline ImPACT™ testing, the facilitation of ‘return to play’ decisions with effective medical treatment, and the development and implementation of a concussion injury surveillance system.
Results: The program has been successfully implemented in about 40 high schools in Miami-Dade County (MDC) over the last two years. The MCM provided baseline testing for 18,357 student-athletes, trained over 100 coaches and 40 athletic trainers, and most recently provided concussion education to high school football athletes. Since 2011, the concussion clinic has treated a total of 216 high school athletes and the surveillance system tracked 198 student athletes.
Conclusion: The MCM aims to assist in the prevention of concussions, improve player safety limiting school liability by providing a countywide concussion management program. The program is funded primarily by private donations and the support of multiple stakeholders. With about 48 States passing concussion legislation, the MCM can be used as a model for other counties to address the need for a concussion management program.
Applications in Sport: Schools with athletic programs need to implement a system to correctly manage and prevent concussive injuries both to protect their athletes and to minimize liability. The development of the MCM and protocol with the support of the leadership of the School Board allows for high schools to take a proactive approach in improving concussion management for their athletes.
INTRODUCTION
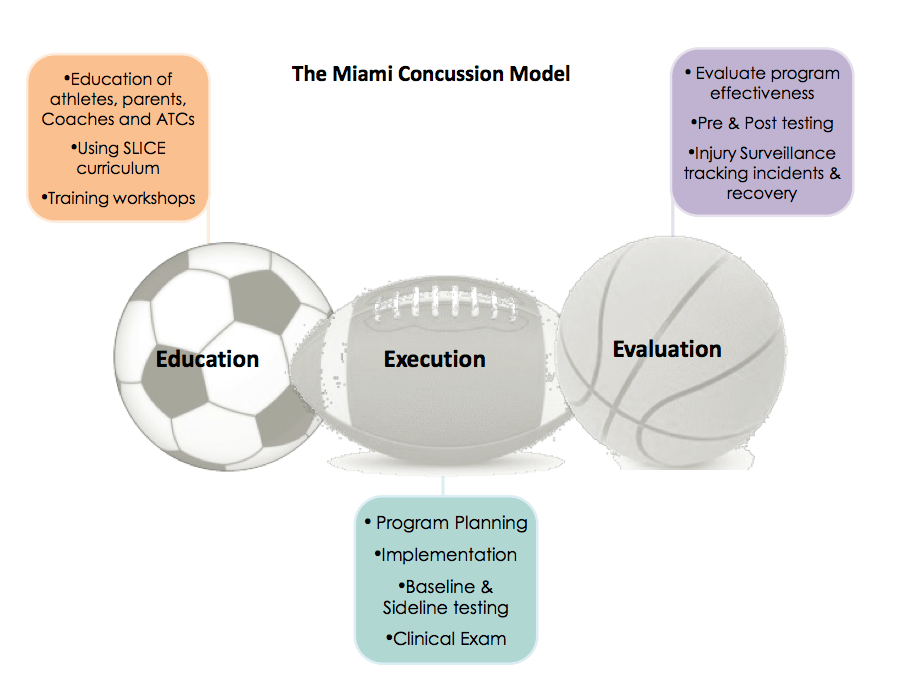
With the national spotlight on concussions in sports, key stakeholders worked together to develop a concussion model, a standard countywide concussion care protocol, and a surveillance system to improve concussion management and to reduce the incidence of sports¬-related concussions at the high school level. In 2011, a student-¬athlete who had sustained multiple concussions playing soccer spearheaded the initiative to create a taskforce to address the management of concussions. A taskforce was implemented consisting of physicians, community leaders, school officials, and concerned parents. The combination of these stakeholders’ backgrounds created a diverse team with unique resources to create a program utilizing a public health approach toward preventing concussions. The Miami Concussion Model (MCM) was designed as a 3-E model (Education, Execution, and Evaluation) outlining phases for program development, implementation, and evaluation (Figure 1).
Figure 1
The program has been successfully implemented in 40 high schools in Miami-Dade County (MDC), baseline testing 18,357 student-athletes over two years. The goals of the MCM are to provide a comprehensive and centralized concussion care program to 1) increase concussion awareness and identification through education and training; 2) facilitate the return to play decision with effective medical treatment which includes baseline neurocognitive testing; and 3) implement a standardized concussion care protocol and concussion injury surveillance system to assist in the prevention of concussions, improve player safety, and limit school liability.
Traumatic brain injury (TBI) is the leading cause of injury¬-related death in children and young adults in the United States and other industrialized countries. A concussion is a type of brain injury caused by a bump or blow to the head that alters cognitive functioning. The Center for Disease Control and Prevention (CDC) has estimated annual sports¬ related concussion incidence is between 1.6 and 3.8 million (Centers for Disease Control, 2010; Coronado et al., 2011; Leibson et al., 2011). Sports is the second leading cause for TBIs after motor vehicle accidents among people aged 15 to 24 years old (Nanda et al., 2012). Studies demonstrate short and long term effects of concussions can be serious and occasionally fatal (Daneshvar et al, 2011; Iverson et al., 2006; Lovell et al, 2003). Most recent public concern has focused on the relationship between Chronic Traumatic Encephalopathy (CTE), a progressive degenerative disease of the brain found in an athlete’s brain post-¬mortem, with a history of multiple symptomatic concussions as well as asymptomatic, repeated sub¬-concussive hits to the head (McKee et al., 2009). As a result of high-profile athletes reporting injuries there has been increased media attention emphasizing the effects of mild traumatic brain injury and concussions in athletes. Beginning in 2009, 48 states nationwide have passed youth sports concussion legislation that requires athletes to be immediately removed from play if a head injury is suspected and then cleared by a licensed medical professional before returning to sport after a head injury.
METHODS
In order to prevent and reduce the consequences of injuries, the CDC recommends the public health approach; describing the problem, identifying the risk and protective factors, developing and testing preventative interventions and strategies, and ensuring widespread adoption of the interventions and strategies (Sleet et al., 2003). This model was used to develop the MCM, a 3E model that includes components of Education, Execution, and Evaluation. The model and the protocol presented in this paper are now being implemented across the county.
Education
The issue of sports related concussions was identified within the MDC community by the University of Miami Concussion Program (UMCP) obtaining accurate injury rates. The number of affected individuals was calculated based on the participation in contact sports in the community. In M¬DC there are 36 public high schools with approximately 15,000 students participating in interscholastic sports annually. M¬DC public high schools had an enrollment of 102,582 students for the 2011¬ and 2012 school years; therefore 14.6% of public high school students in MDC participated in sports and were affected/at risk for sports¬ related concussions. This excluded the students that participated in physical education courses who were also at risk (Miami-¬Dade Public Schools Research Services [M-DPSRS], 2011). As perceptions regarding concussion started to change in the county and awareness increased due to media attention, M¬DC school officials became open to discussion to improve their concussion management plan. This allowed for meetings with key personnel involved with high school athletes (athletic directors, coaches, athletic trainers, physical education teachers, etc.). These meetings were very important in that they revealed their knowledge and their experience with sports concussions and their thoughts of how to improve management for their athletes.
Review of existing sports concussion management protocols and resources in the community was conducted to 1) determine if any current concussion management programs or plans existed, 2) obtain information from local emergency rooms and physicians’ offices relevant to concussion planning, and 3) identify how those individuals managed concussion in youth sports and where they were referring their patients for specialized follow-¬up care. That information taken from multiple sources (leagues, parks, schools, state laws, and local medical care centers) was summarized regarding the issue of sports concussions within the community. For example, most high school aged (13-19 years) students in the community participated in interscholastic sports versus park recreational leagues; the majority of injuries occur between the months of August and January during football season because football teams have the largest number of athletes. Being well informed on the issues of concussion management allowed a focused approach toward building a concussion care program for the community via the MCM.
The UMCP was then able to identify the weaknesses in each phase of concussion management and propose resolutions to strengthen each area. A community task force was developed that consisted of key stakeholders from different agencies involved in concussion management. This included school board representatives, first responders to the injury, medical providers, and community leaders.
Most recently UMCP has partnered with the Sports Legacy Institute and joined their community education program through their Sports Legacy Institute Community Educator Program (SLICE). SLICE is a fun, interactive concussion education program that teaches young student-athletes about concussions through discussion, video, and interactive games (Sports Legacy Institute [SLI], 2013). Currently, a modified version of SLICE, which is a 30-minute power point presentation, is being used to educate high school football players.
Support and approval for concussion planning was obtained from the various constituencies for the community task force and was followed up with research of each district, county, and state policy pertaining to sports concussions for high school athletes. Verification of regulations was implemented and continuously updated to allow consistency with the newest management protocols as outlined in the Consensus Statement from the International Committee on Sports Concussions (McCrory et al., 2008). Legislation has passed in 48 states across the country requiring student athletes to receive written medical clearance before returning to the playing field. These state laws include the requirement that athletes, parents, and coaches receive concussion education. Prior to 2011 limited regulations existed in the MDC community, so the UMCP collaborated with school board officials to formulate a plan to involve relevant personnel from the athletic department. In MDC, the school board’s Director of Athletics assisted with the planning and implementation as one of the critical task force members, her cooperation and support ensured feasibility and assistance with the school board approval. The UMCP worked directly with the schools and school board to improve the success of developing a standard program that could reach all athletes. In M¬DC Public Schools, each school has a certified athletic trainer (ATC) that works full-time at his/her school and is an employee of the School Board. The unique qualifications of ATCs made them the most appropriate person to collaborate with upon implementing the program in each school. The Director of Athletics for MDC public schools supported these efforts and began communication between UMCP and the ATCs. Even where certified athletic trainers are not readily available, athletic coaches or the school nurse were trained to implement the program. In March 2011 the ATCs and Coaches were provided with a comprehensive Concussion Management and Training Workshop by UMCP.
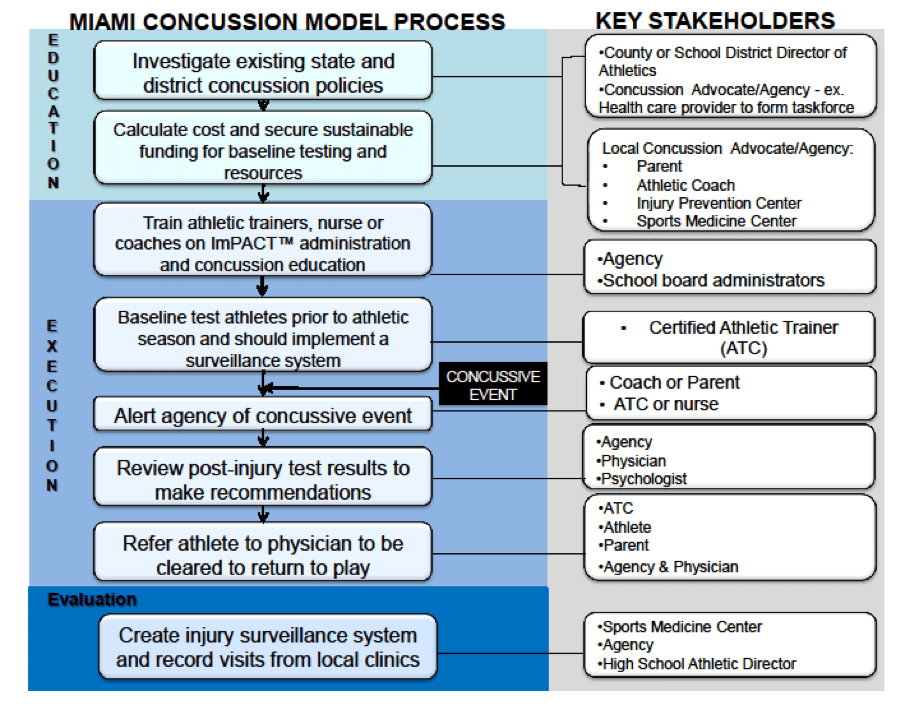
Finally, a plan was developed for funding and sustainability of the program. The first step was to review any existing funding mechanisms and potential new resources to support the implementation of a comprehensive management program. The plan included 1) staff/operations costs and baseline neurocognitive testing for all student athletes; and 2) implementing the centralized concussion care program as an investment in the safety of athletes that improves the prevention of concussions¬¬ by facilitating ongoing training and education which reduces liability when administered properly. However, in most public school systems budgets do not include a plan for concussion prevention/care, and funding can be difficult to find. The cost of operating such a program will vary depending on the size of the school district and the structure of the program. The process described (see Figure 2) demonstrates the development of an infrastructure for operation of the model. In MDC it was feasible for the UM Concussion Program under the KiDZ Neuroscience Center (KNC), which is a center devoted to improving the quality of care and advances in research and prevention of traumatic and acquired brain and spinal cord injury in children to partner with the MDC Public School Board. Additionally, since the MDC school board employs their own ATCs, training was provided for baseline neurocognitive testing of athletes playing contact sports and was added to their existing duties. In M¬DC, ImPACT™ (Immediate Post-Concussion Assessment and Cognitive Testing) is utilized because it is an evidence ¬based assessment that has been widely used and validated (Schatz et al., 2006). ImPACT™ is a 20-minute online computer exam consisting of five sections that assess memory, reaction time, non-verbal and verbal problem solving, and attention span. Baseline ImPACT™ scores are valid for four years for each athlete during their high school years, which reduces the annual cost of purchasing new exams. UMCP receives a charitable donation from a private high school annually that covers the price of purchasing baseline tests by volume for reduced pricing for all 36 public high schools in the county. The private schools buy their own licenses. The Director of the UMCP is also a Credentialed ImPACT™ Consultant with training that coordinates all the baseline testing. If an athlete sustains a concussion then they are retested by the ATC within 48-72 hours and the Director of the UMCP is notified and recommendations made and clinic visits scheduled.
Figure 2
Execution
Once approval by the different agencies was granted, the execution phase of the MCM was initiated. The Countywide Concussion Care Protocol was developed to create a standard protocol for the concussion management of high school athletes (Figure 2). The first phase involved training and educating appropriate staff about concussions in sports and also how to administer baseline neurocognitive tests. The ATCs and school nurses were educated about concussion management and worked closely with an expert in concussion management to provide accurate information and to respond to questions. Prior to this program the Director of the UMCP taught a mandatory educational and training workshop for ATCs and Coaches that was expanded and continues. Other school professionals like nurses that may be involved in management of care for student athletes are trained annually on the concussion protocols as guidelines and recommendations change. In MDC, sideline assessment requirements include the Sports Concussion Assessment Tool 2 (SCAT2) and the King-Devick Test. The SCAT2 represents a standardized method of evaluating athletes aged 10 and older for concussion injuries through a series of cognitive questions and physical assessments (McCrory, 2009). The King-Devick Test is a rapid visual screening tool that is used to confirm suspected concussions, the athlete is asked to read numbers from the cards in sequence without errors as fast as possible. The athlete’s post-injury performance is compared to their pre-season baseline result (Galetta et al., 2011). Both of these assessments are utilized on the sidelines to verify suspected concussion symptoms and provide an objective confirmation of the injury. Protocols and guidelines are reviewed and updated annually to be consistent with national and state requirements and the latest medical research recommendations. During the pre¬-season training workshop by the UMCP, ATCs were trained on evaluating and administering baseline assessments to athletes. Two assessments require baseline results, ImPACT™ and the King-Devick test; athletes are tested prior to the start of contact drills to obtain accurate baseline results. In MDC, a list of testing guidelines was created for the school staff to reference throughout the year. After all athletes are tested, the ATCs, coach, or nurse contact the Director of the UMCP to verify that all baseline tests are valid before athletes are introduced to contact activities.
The MCM incorporates medical evaluation of the concussed athlete. UMCP works in conjunction with local physicians and other psychologists to assess the physical and neurocognitive consequences of the injury. The athletes receive comprehensive medical care, which is mandatory for clearance to play. UMCP provides a comprehensive concussion management program assessing the athlete’s medical, cognitive, and psychological well being during the recovery process. The pressure that athletes have to return to their pre¬-morbid academic and athletic levels can be overwhelming for an adolescent, particularly when their peers cannot understand the extent of their injury. The ImPACT™ neurocognitive computer test results coupled with a thorough clinical assessment aids the medical team in making an accurate prognosis and providing the athlete with confidence when returning to play. The UMCP medical team works directly with the ATCs to communicate the status of the athlete’s recovery.
Evaluation
When evaluating the model UMCP researchers examined individual school compliance as well as overall effect of program implementation on head injury rates in the county. The concussion protocol dictates that a school staff member will document the athlete’s immediate symptoms and details of the injury incident, which can be seen in Figure 2 (Evaluation). The ATC, coach, or nurse is to document each incident and keep accurate records, including: sideline assessment results from the Sports Concussion Assessment Tool 2 (SCAT2) or the King¬-Devick test (McCrory et al., 2008). Within 24¬-72 hours of the injury the athletic trainer, coach, or nurse would have administered a post¬-injury test to the injured athlete, reported the incident to the program coordinator and sought medical attention for the athlete.
Various methods to collect data can be utilized including tracking patients in local clinics and emergency departments, integrating an injury reporting system and continued follow-¬up with the school personnel. In MCM the records of concussion patients treated at UMCP are collected and an online concussion injury surveillance tool has been developed. The online injury¬ reporting form collects relevant details of the concussive incident including age, gender, sport, mechanism of injury, history of concussion, equipment that was worn at the time of injury, and geographical region within the county. It is necessary to collect accurate data surrounding each injury to better identify the specific issues occurring whether it is equipment failure, environmental, incorrect coaching, etc. The involved agencies collaborated to evaluate the effectiveness of the program after its implementation.
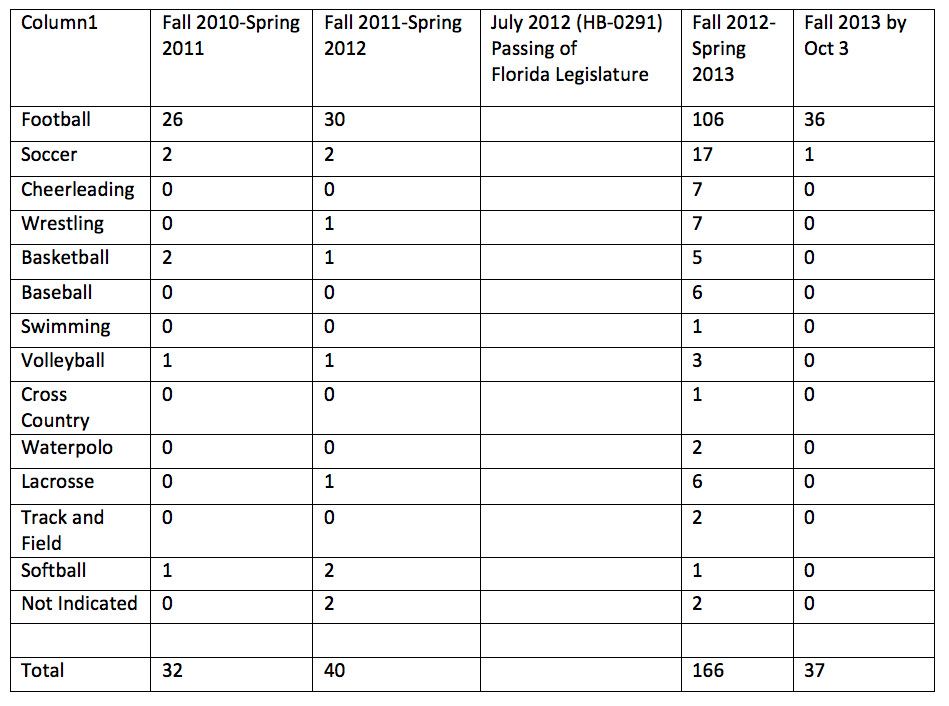
The Florida State Legislature passed House Bill 0291 in July of 2012 to ensure there are policies relating to the nature and risk of concussion and head injury in youth athletes requiring informed consent for participation in practice or competition and removal from practice or competition under certain circumstances, and written medical clearance to return. Pre-Legislation data from concussions reported in High School Sports based on age, sex, and ethnicity were obtained through the surveillance system. The pre-legislation results for all sports at 36 MDC High Schools for the 2010-2011 school year reported 32 concussions. For the following school year 2011-2012, still reported as pre-legislation, 40 concussions were reported. The most significant increase in reporting was for the school year 2012-2013, which was post-legislation data obtained after the passing of HB 0291 in July 2012. The 2012-2013 school year reported 166 concussions, a four-fold increase in concussion reporting. (Table 1)
Table 1. Surveillance Data
Concussion reporting for all sports in 36 Miami-Dade County Public High Schools
The marked increase in reporting after the implementation of HB-0291 is attributed to increased awareness and the addition of a standard management protocol. The program has been successfully implemented in about 40 high schools (36 public and 4 private) in MDC. The MCM provided ImPACT™ baseline testing for 18,357 student-athletes, trained over 100 coaches and 40 athletic trainers, and most recently provided concussion education to high school football athletes. Data obtained from the UMCP clinic reports that in 2010, prior to the implementation of the standard protocol, 44 high school athletes from both public and private schools were treated for sports concussions during the fall athletic season (August-¬January). In 2011, post¬-implementation of the model, 61 athletes sought treatment for concussions. During the 2012 fall season and up to the present time, 155 ¬athletes were treated in the same clinic for a sports-¬related concussion, which included all sports for a total of 216 athletes treated. There are some athletes that return to their pediatricians or family doctors for their care and for clearance for return to play however the ATC at their school still follows the protocol and will enter data in the surveillance system. The chief complaints that athlete’s reported during clinic visits included; headaches, dizziness, fatigue, visual disturbance, and concentration issues. Most of these physiological symptoms were accompanied by cognitive deficits, which affected their academic performance. The clinic has developed a protocol for gradual return to play which includes exertion activities from low to high as tolerated and also return to class and academic work with specific accommodations. The University subjects’ review board approvals were obtained prior to collecting any data. The majority of the concussive injuries occurred in an MDC high school setting or at a school¬ sanctioned athletic event. In 2012, 198 high school concussion injuries were reported through a concussion injury surveillance system that the ATCs have been trained to use, 183 (92.4%) of those reported incidences occurred at a school or at a school sponsored athletic event.
DISCUSSION
The MCM presented here was implemented in MDC in 2011. From this pilot evaluation of the model it was determined to be effective in increasing the number of concussions identified, reported, and also treated at the UMCP clinic. Also a centralized standard protocol was now in place across the county allowing for better communication and compliance for reporting by the high school ATCs. This model, or a modified version, can be implemented to centralize concussion management in other counties and communities across the country. There is a unified need in every community for the development of concussion care protocol with the ever-increasing awareness and liability involved in high school sports.
CONCLUSION
Concussions affect all aspects of the student-¬athlete and therefore management of an injured athlete should be comprehensive and include psychological assessments, neurocognitive testing, academic support, and a physiological examination. A comprehensive program that combines education, baseline neurocognitive testing, clinical care and evaluation is believed to be most beneficial to maximize the effectiveness of such a program. The MCM outlined in this paper is designed to be a guideline that can be adapted to the needs of different communities. Data will continue to be collected and analyzed to evaluate the effectiveness of this program. With limited coordination and low cost for baseline testing it is important to have a concussion management program in place.
BARRIERS TO IPLEMENTATION
Since the MCM was developed with the consensus of key stakeholders, there has been little resistance. The model presented has recently been developed and is going through continual evaluation. While the preliminary data seems promising, we will continue to evaluate this model over the next few years. Since the identification of a concussive event relies on the reporting of injuries by the ATCs at each high school their support and implementation of the program is critical in the success of the program. The staff of the UMCP suspected that the number of concussive injuries was still under¬reported in the first year, however now with the passing of the Concussion Legislation in July 2012, reporting has increased. Also with continued training and education workshops and the centralized system this should improve compliance. Since MDC has ATCs that all work for the school board it is much easier to implement such a program. In other cases where the ATCs work for medical or rehab facilities they need to be compensated for their time in supervising and administering of the baseline ImPACT™ testing. If they are not able to participate a school nurse could be trained. Funding for the MCM will continue through a commitment made by the fundraising efforts of one private school in MDC, however there are other ways to budget for such a program; Parent¬ Teacher Association fundraisers, booster club events, corporate support, local sports teams sponsorship, or a nominal fee inclusive in yearly athletic dues.
APPLICATIONS IN SPORTS
The increased awareness of concussions and their effects on the developing brain have created a culture change in sports. Schools with athletic programs need to be encouraged to implement a system to correctly manage and prevent concussive injuries both to protect their athletes and to minimize liability. The development of the MCM and protocol with the support of the leadership of the School Board allowed for the high schools in MDC to take a proactive approach in improving concussion management for their athletes. The Baseline neurocognitive computerized testing ImPACT™ provided an objective measure that with the clinical exam assisted in determining a beneficial recovery plan for the athlete and providing a plan for the school to limit their liability while better caring for their student-¬athletes while identifying and preventing injuries.
ACKNOWLEDGMENTS
The authors would like to thank Dr. Kaplan and the UHealth Sports Medicine Clinic and Staff, also Cheryl Golden, Director of Athletics for the Miami-Dade County School Board and all the Miami-Dade County Certified Athletic Trainers. We would also like to thank Ransom Everglades School, David Goldstein and the Goldstein Family for their initial and continued support of the UMCP.
REFERENCES
1. Centers for Disease Control. (2010). National Center for injury prevention & control: Traumatic brain injuries. Heads up: Concussions in high school sports. Retrieved from http://www.cdc.gov/concussion/sports/index. html
3. Daneshvar, D.H., Riley, D.O., Nowinski, C.J., McKee, A.C., Stern, R.A., & Cantu, R.C. (2011) Long¬term consequences: Effects on normal development profile after concussion. Physical Medicine and Rehabilitation Clinics of North America, 22(4), 683-700.
4. Galetta, K.M., Brandes, L.E., Maki, K., Dzuenuabwucz, M.S., Laudano, E., Allen, M.,…Balcer, L.J. (2011). The King¬-Devick test and sports related concussion: Study of a rapid visual screening tool in a collegiate cohort. Journal of Neurological Science, 309(1¬2), 34¬-39
6. Leibson, C.L., Brown, A.W., Ransom, J.E., Diehl, N.N., Perkins, P.K., Mandrekar, J., & Malec, J.F. (2011). Incidence of traumatic brain injury across the full disease spectrum. Epidemiology. 22(6), 836-¬844.
7. Lovell, M., Collins, M., Iverson, G., Field, M., Maroon, J., Cantu, R., & Podell, K. (2003). Recovery from mild concussion in high school athletes. Journal of Neurosurgery, 98(2), 296-¬301.
8. McCrory, P. (2009). Sport concussion assessment tool 2. Scandinavian Journal of Medicine and Science in Sports, 19(3),452-452.
9. McCrory, P., Meeuwisse, W., Johnston, K., Dvorak, J., Aubry, M., Molloy, M., & Cantu, R. (2009). Consensus statement on concussion in sport – the 3rd international conference on concussion in sport, held in Zurich, November 2008. Journal of Clinical Neuroscience, 16(6), 755-¬763.
10. McKee, A., Cantu, R., Nowinski, C., Hedley-Whyte, E.T., Gavett, B.E., Budson, A.E.,…Stern, R.A. (2009). Chronic traumatic encephalopathy in athletes: Progressive tauopathy following repetitive head injury. Journal Neuropathology and Experimental Neurology, 68(7), 709-735.
11. Miami-¬Dade Public Schools Research Services. (2011) Statistical Highlights, 2010-2011[Data File]. Retrieved from http://home.dadeschools.net/files/Statistical Highlights.pdf.
12. Nanda, A., Kahn, I.S., Goldman, R., & Testa, M. (2012). Sports Related Concussions and the Louisiana Youth Concussion Act. The Journal of the Louisiana State Medical Society, 164(5), 246-250
13. Schatz, P., Pardini, J.E., Lovell, M.R., Collins, M.W., & Podell, K. (2006). Sensitivity and specificity of the ImPACT Test battery for concussion in athletes. Archives of Clinical Neuropsychology, 21(1), 91-99.
14. Sleet, D.A., Hopkins, K.N., & Olson, S.J. (2003). From Delivery to Discovery: Injury Prevention at CDC. Health Promotion Practice, 4(2), 98-102.
15. Sports Legacy Institute. SLI Community Educators (2013). Retrieved from http://sportslegacy.org/education/slice.